What is temporal or temporal arteritis
It is still not known for certain what exactly gives impetus to the development of the disease. But the mechanism of the disease does not depend on the cause. It was studied in the first half of the 20th century by the American scientist Horton, who gave the disease its second name.
The pathological functioning of the immune system leads to the formation of antibodies, which begin to attach to the walls of large arteries. As a result, inflamed clusters of cells – granulomas – appear. In these foci, lymphocytes, plasma cells, histiocytes and huge multinucleated cells characteristic of the disease are found. It was they who gave another name to the disease - giant cell arteritis.
There are several theories explaining the appearance of vascular disease. Among the provoking factors, scientists identify heredity, previous infectious diseases, and age-related changes. But so far none of the hypotheses have been proven.
Due to the occurrence of local edema, the lumen of blood vessels decreases, which means that blood circulation sharply decreases and an environment for the development of blood clots appears. As a result, the patient faces blindness, ischemic stroke, and aneurysm.
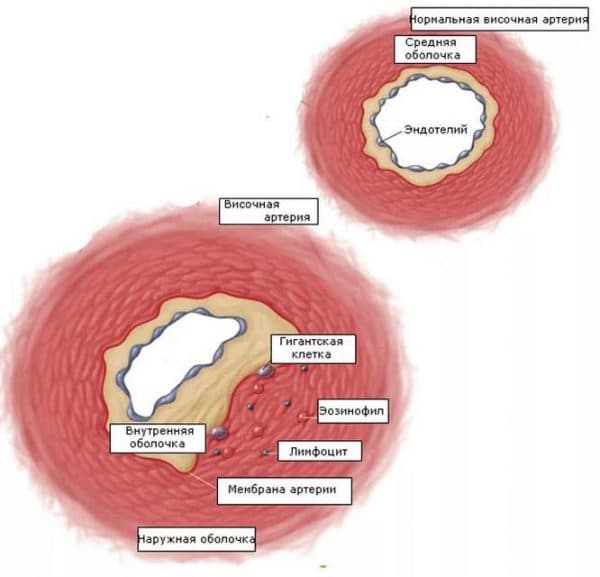
The affected vessels have a small lumen
The article will tell you what swelling of the upper eyelid indicates.
Causes of the disease
Researchers have not been able to reliably establish the causes of the development of this disease.
It is believed that the cause may be a genetic predisposition. In addition, by the fact that people get sick more often after 50 years of age, one can judge the role of hormonal and age-related changes in the occurrence of Horton's disease. Temporal arteritis is characterized by systemic damage to the arterial bed with a peculiar localization of affected areas and the presence of giant cells in the infiltrate. During the development of the disease, any arterial bed can be affected, but in almost all cases changes are found in the aorta and large vessels extending from it. The smaller the caliber of the artery, the weaker the signs of inflammation.
Symptoms of the disease
Arteritis is most often diagnosed in people over 60 years of age, mainly women. The onset of the disease is characterized by a deterioration in the patient’s general well-being and weight loss. He may experience muscle soreness, a slight increase in temperature, decreased appetite, weakness and nausea. The longer this period lasts without other manifestations (and it lasts up to several months), the easier the course of the disease is predicted.
The lesion begins in the aortic arch, gradually spreading through the circulatory system. The temporal, ophthalmic, and vertebral arteries are most often affected.
You can find instructions for Vial eye drops here.
Visual symptom of the onset of the disease
Over time, the patient begins to suffer from an aching or throbbing headache. It gets worse at night or while chewing. Most often, unpleasant sensations are localized in the forehead and crown, but sometimes they radiate to the back of the head, neck, and shoulder.
On the part of the damaged artery, pain gradually appears when combing or touching the hair. Redness and swelling may appear at the temple. In addition, the functionality of facial muscles decreases - it is difficult for the patient to talk or chew.
The disease causes complications in the eyes. There may be a sharp deterioration in vision, double vision, pain in the apples, and the upper eyelid droops.
A characteristic sign of arteritis is bulging and tortuosity of the temporal vessel. The pathology is noticeable to the naked eye, and when pressed, a painful pulsation is felt.
Damage to various arteries leads to other associated symptoms - morning muscle stiffness (polymyalgia), angina pectoris, attacks of weakness. In severe cases, gangrene of the scalp and necrosis of the limbs develop.
Lack of treatment can lead to disability and even death for the patient
Reasonable savings or a dangerous experiment on your own - analogues of Vigamox eye drops.
Description and types of disease
The disease was first studied and described by the American physician Horton in the 30s.
XX century There are primary and secondary temporal arteritis. In the first case, arteritis develops as an independent disease, more common in older people. Granulomas are rarely of infectious origin. Secondary arteritis is the result of an atypical response of the immune system to an infection or virus if the disease is severe. The disease affects the main and middle vessels. More often, the pathology is localized in the area of the carotid artery and aorta. The vessels are responsible for supplying blood to the back of the head, temples, and eye areas - these areas are mainly affected by negative symptoms. Types of Horton's disease depending on symptoms:
- classic – the temporal artery is affected;
- latent – signs of damage can only be established by biopsy, the disease is asymptomatic;
- damage to the blood vessels of the eyes;
- with a predominance of nonspecific symptoms.
The disease is autoimmune in nature, lymphocyte cells accumulate and become inflamed, the process can become chronic. The vascular walls are infiltrated, and cellular accumulations form in the foci of inflammation. The surface of the vessels becomes uneven, the process of damage to the arteries is uneven. Over time, the lumen narrows, there is a lack of blood supply, oxygen starvation of organs and tissues. Arteritis is a rheumatic disease that worsens the patient’s quality of life. Headaches worsen at night - the patient is in a state of stress and cannot get enough sleep and rest.
Important! ICD code is B08.
Diagnostic features
To identify arteritis, consultation with a rheumatologist is required. During the examination, the doctor can identify areas of thickening of the veins and their increased sensitivity. The patient's medical history is supplemented with relevant complaints.
MRI is a reliable diagnostic method
The results of a general examination are unthinkable without the results of a blood test. In the presence of temporal pathology, the following anomalies will certainly be detected:
- high level of ESR and decreased number of red blood cells;
- presence of C-reactive protein;
- moderate anemia.
Since the pathology sometimes develops rapidly and the consequences can be very severe, therapy is often started before all diagnostic procedures are completed.
Additionally, the doctor may prescribe an ultrasound and angiography to see the picture of vascular changes.
But all these methods indirectly indicate the disease. The diagnosis is confirmed by a biopsy, during which a small section of the temporal artery is examined. If the sample contains an inflamed lesion, the multinucleated cells found confirm the suspicions.
Read how to treat viral keratitis here.
The headache is unbearable
To ensure the safety and effectiveness of the prescribed therapy for allergies, read the instructions for using Visallergol eye drops.
Symptoms
Arteritis symptoms are usually of a general nature, and they appear before the onset of specific symptoms:
- chills;
- general weakness;
- refusal to eat;
- hyperhidrosis;
- myalgia;
- sudden weight loss.
Signs indicating the occurrence of this pathology are as follows:
- there is a disturbance in the blood flow to the brain;
- sometimes loss of consciousness occurs;
- Cases of stroke are not uncommon.
The most common diagnosis is arteritis of the temporal artery. It has its own symptoms.
So, temporal arteritis exhibits the following symptoms:
- constant headache;
- the artery at the temples swells, becomes painful, and the pulsation in it weakens.
Head pain occurs in almost all patients. This is the first sign of diffuse pathology. When palpating the affected arteries, a person experiences severe, spreading pain. Vessels that have become inflamed become thicker and begin to twist. The skin over them turns red and swelling forms.
With temporal arteritis, pain occurs in the temples, radiating to the neck, shoulder, and lower jaw. There is a throbbing pain that intensifies while chewing food. Vision deteriorates, eyelids droop, and double vision appears. The muscles weaken, this condition has its own name - arteritis with rheumatic polymyalgia. The pathology is characterized by stiffness of the muscles of the limbs, pelvis and shoulders.
When arteritis of the facial artery or maxillary artery occurs, pain appears in the masticatory muscles, teeth and tongue. In addition, it is accompanied by muscle numbness. There is severe pain under the jaw, which reaches the nasolabial triangle and the corners of the eyes. It indicates poor blood flow to this muscle.
Digital arteritis involves death of the soft tissue under or around the nails. If the vessels of the brain are affected, corresponding signs will appear.
Ophthalmological risks
Even at the diagnostic stage, regardless of complaints, you need to visit an ophthalmologist. The fact is that the disease almost always affects the arteries leading to the organs of vision.
The disease often begins to develop on one half of the body, respectively, only the right or left eye is affected. But in 30% of cases there is a bilateral decrease.
As a result of the development of pathology, several complications may appear at once:
- if the nutrition of the arteries of the optic nerve is disrupted, the patient observes a sharp decrease in acuity, deterioration in peripheral visibility;
- in cases affecting the retinal vessels, loss of vision occurs, reducing its quality up to complete loss;
- in the future, nerve paralysis is likely, causing disturbances in eye movements, double vision and ischemic syndrome;
- There are frequent examples of retinal edema, cataracts, hemorrhages, and increased intraocular pressure.
Arteritis is dangerous because if the eyes are affected, the patient may not observe other signs of the disease for a long time. Therefore, the presence of vision complaints in old age requires a mandatory visit to the doctor. In turn, the specialist, seeing vascular disorders, should check for suspicions of temporal arteritis. Timely diagnosis and treatment will help avoid irreversible consequences.
Read here how to determine color blindness.
Corticosteroid is an effective treatment for autoimmune diseases
Find out when Visomitin eye drops will help here.
Horton's arteritis
- Etiology
- Classification
- Clinical picture
- Diagnostics
- Treatment
Horton's disease (temporal/cranial/giant cell arteritis) is a granulomatous vasculitis of the aorta and its main branches (mainly extracranial branches of the carotid artery) with frequent involvement of the temporal artery. GCA is the most common primary vasculitis in adults, almost exclusively over 50 years of age. The incidence in this population is about 18 per 100 thousand people per year and increases with age, reaching a peak in the 8th decade of life.
In recent years, the incidence has increased slightly, which is associated with improved awareness among doctors about this disease and, accordingly, with improved diagnosis. Data on the structure of long-term morbidity indicate that there is a cyclical pattern - an increase in morbidity occurs every 7 years. If we consider the seasonal cycle, the peak occurs in October-November and April-May. The ratio between men and women is 1:1.5-2.
An example of a diagnosis formulation
Horton's arteritis with damage to the left superficial temporal artery, polymyalgia rheumatica, exacerbation. Complications: right-sided amaurosis; aneurysm of the aortic arch (4 cm).
Prevention has not been developed. No screening is carried out. Screening with duplex ultrasound of the superficial temporal artery is theoretically possible in the following situations:
- fever of unknown origin in persons over 50 years of age;
- increased ESR of unknown origin in people over 50 years of age;
- new severe headaches in the temporal region in people over 50 years of age;
- persons over 50 years of age with unmotivated weakness of the masticatory muscles.
Horton's arteritis occurs most often in Scandinavian countries, less often in Spain and Italy, and extremely rarely in African countries and among people from there.
Etiology
Various infectious agents are considered as possible etiological factors for Horton's arteritis. An infectious etiology is supported by a seven-year cyclicity, as well as some intra-annual cyclicity. As a result of numerous studies, three pathogens have been identified, the presence of which is most often associated with the development of the disease: Parvovirus B19, Chlamydia pneumoniae, Human parainfluenza virus type 1.
In a third of patients, HBsAg and antibodies to it are detected; HBsAg is also detected in the wall of the affected arteries. There is a genetic predisposition (family aggregation, carriage of HLA B14, HLA B8 and HLA A10, carriage of DR4 has been established).
The main mechanisms of the pathogenesis of Horton's disease are
- vessel stenosis caused by intimal hyperplasia;
- neoangiogenesis-induced intimal proliferation;
- peroxide damage to medial smooth muscle cells;
- activation of smooth muscle cells by oxidative damage;
- secretion of interferon α (IFNα), the main regulatory cytokine of damage;
- early involvement of adventitial dendritic cells in arteritis;
- innate immune response directed at systemic inflammation;
- systemic inflammation, often preceding isolated vascular inflammation.
Immunological disorders play a leading role in the pathogenesis. Antibodies to immunoglobulins G, A, M and C3 fractions of complement, deposition of immune complexes in the intima of the vessel and in the elastic layer are detected. Transmural arterial disease induces luminal occlusion through intimal hyperplasia. An important role is played by cell-mediated immune reactions directed against arterial wall antigens, which determine the granulomatous nature of cellular infiltrates. It should be noted, however, that the information available today is of little evidence and the etiology of this vasculitis cannot be considered established.
There is evidence that the middle layer of arteries (media) is a kind of antigen storage in which the antigen is retained, even despite its elimination from other tissues. Antigen persistence leads to the development of an interferon-γ-dependent inflammatory response. These data were obtained in a mouse model of herpes-associated vasculitis affecting large arteries. The general pathogenesis of Horton's arteritis is similar to another giant cell vasculitis - Takayasu's arteritis.
Classification
Manifestations of GCA span a wide range of clinical subtypes. Among them are cranial GCA with severe ischemic complications (vision loss, cerebral ischemia, etc.), arteritis of large vessels (subclavian and axial stenosis), aortitis (aneurysm and/or rupture of the aorta), systemic inflammatory syndrome with non-stenosing vasculitis, as well as “ isolated" polymyalgia rheumatica with myalgias, depression, fatigue, anorexia and subclinical systemic vasculitis. There are descriptions of GCA with damage to the aorta and pulmonary artery with occlusion of one of its branches, involving the arteries of the arms and legs (from 3 to 16%), necrosis of the tongue, dry cough and other localizations
Horton's arteritis is a primary systemic vasculitis. If we classify primary systemic vasculitis according to the size of the affected vessels, the presence of granulomas and areas of necrosis, and the determination of antibodies to the cytoplasm of neutrophils (ANCA), then Horton's arteritis will be in the same group with Takayasu's arteritis.
Horton's arteritis is usually divided into the classic version (involving the branches of the external carotid artery) and the version with damage to large arteries : subclavian, vertebral and even iliac (Takayasu-like variant - 15% of cases).
Depending on the ESR value, an inflammatory form (with an increased ESR) and a non-inflammatory form (with a normal ESR) are distinguished.
Clinical picture
The onset of the disease can occur in different ways. The following types of complaints can be distinguished.
- “vascular” symptoms - “classic triad” (temporal arteritis, visual impairment, polymyalgia rheumatica)
- “rheumatological” symptoms - stiffness, pain in the muscles and joints of the shoulder and pelvic girdles.
- “general therapeutic” symptoms - fever, weakness, loss of appetite, weight loss, headache. In this case, headache (one of the most common and characteristic symptoms) is localized in the temporal region, along the branches of a. temporalis superficialis, but can bother both the frontal and occipital regions. The intensity of pain varies from slight to very severe. It is important to pay attention to the absence of similar headaches in the past.
- “ophthalmological” symptoms - occur in a third of patients. These disorders are described in more detail below.
The following symptoms are important for making a diagnosis:
- “lameness of the lower jaw” - weakness and rapid fatigue of the masticatory muscles (patients note that they cannot chew for a long time, some patients complain of pain in the tongue);
- pain at the site of palpation a. temporalis superficialis (seen in approximately 30% of patients).
The appearance of unilateral headaches or a change in the nature of the “old headache” is the most common symptom of Horton's arteritis.
| Symptom | Frequency at the onset of the disease, % | Frequency at the height of the disease, % |
| Headache | 86 | 90 |
| "Lameness of the lower jaw" | 64 | 67 |
| Temporal artery change | 40 | 50 |
| Polymyalgia rheumatica | 21 | 50 |
| Vision disorders | 35 | 40 |
| Fever | 19 | 21 |
Horton's arteritis can manifest itself with the most unexpected symptoms. It should be noted that not all patients with atypical manifestations of the disease have classic symptoms.
Relatively rare symptoms include:
- cough;
- glossitis;
- infarction of the larynx and/or tongue;
- a sore throat;
- aortic aneurysm (including dissecting aneurysm);
- lameness of the limbs;
- Raynaud's phenomenon;
- peripheral neuropathy;
- dementia, transient ischemic attacks, stroke;
- myocardial infarction;
- tumor formation in the breast or ovary;
- syndrome of inappropriate secretion of antidiuretic hormone;
- microangipathic hemolytic anemia.
There are three forms of Horton's arteritis:
- classic version: inflammatory form - fever, weakness, weight loss, increased ESR, increased IL-6 activity;
- form of Horton's arteritis with normal ESR - absence of symptoms characteristic of the inflammatory form; high hematocrit; normal ESR; increased risk of vision loss, skin necrosis of the temporal region and other ischemic complications;
Organ lesions
Organ damage directly depends on vascular damage and is almost always only ischemic in nature.
Depending on the frequency of involvement, three groups of vessels are distinguished.
- often affected (extracranial branches of the carotid artery) - a. temporalis superficialis, a. masseterica, a.lingvalis;
- rarely affected (arteries of the extremities) - a. subclavia, a. axillaris, a. iliaca interna, a. femoralis;
- extremely rarely affected (visceral arteries with the exception of a. carotis interna, a. vertebralis) - aa. coronariae, truncus caeliacus, a. mesenterica superior, a. renalis.
If the internal carotid artery is involved in the pathological process, then the most common symptoms are associated with damage to the central nervous system: dizziness, headaches (not associated with damage to the superficial temporal artery). Transient ischemic attacks can sometimes result in a stroke.
Ophthalmological disorders occur in 14-70% of patients and the cause of such problems in most cases is ischemia a. ciliary posterior, a. ophthalmica. Partial or complete loss of vision is the most serious complication of Horton's arteritis. Amaurosis can be either unilateral or bilateral. This complication develops suddenly and, as a rule, is permanent. With anterior ischemia of the optic nerve, amaurosis fugax can develop. Other ophthalmological complications: ophthalmoplegia, Horner's syndrome, diplopia, eye pain.
According to recently published results of a retrospective study (Loddenkemper T., Sharma P. et al., 2007), which examined risk factors for visual impairment in Horton's arteritis, papilledema and arterial hypertension are the leading predictors of early (during the first weeks of the disease) loss of vision.
Diagnostics
Particular attention should be paid to examination and palpation of the temporal arteries, which reveals their thickening and soreness, and redness of the skin over them. During auscultation, murmurs may be heard over the carotid, brachial or axillary arteries, in the supraclavicular region.
Patients with polymyalgia rheumatica may experience limited movement of the neck, shoulder and hip joints, which is associated with pain. The shoulders may be painful on palpation. In some patients (15-20%), synovitis of the hands or knees is detected.
Diagnostic criteria
Clinically relevant diagnostic criteria for Horton's arteritis have not yet been developed. The classification criteria of the American Rheumatological Association (American College of Rheumatology) are often used, but it must be remembered that they were developed to differentiate systemic vasculitides from each other in clinical trials and have not been evaluated in real-world clinical settings.
- Age of onset over 50 years—development or onset of symptoms in individuals over 50 years of age.
- “New” headache is the development of a new or change in the previous location of the headache.
- Pathology of the temporal artery - pain in the temporal artery during palpation or a decrease in pulsation, not associated with atherosclerosis of the vessels of the neck.
- Increase in ESR >50 mm/h using the Westergren method.
- Biopsy-proven pathology of the arterial wall - morphological examination of biopsy material from the arterial wall shows vasculitis, characterized predominantly by mononuclear infiltration or granulomatous inflammation, usually with multinuclear giant cells.
To make a diagnosis of Horton's arteritis, three of the five criteria must be met. Sensitivity is 93.5%, specificity is 91.2%.
Determination of disease activity
To assess the activity of Horton's arteritis, use:
- Birmingham Vasculitis Activity Score (Birmingham vasculitis activity scale);
- interleukin-6 concentration.
There is no correlation between the ESR value and the activity of Horton's arteritis. It is possible that the generalized (Takayasu-like) form of Horton's arteritis involving the subclavian and other large-caliber arteries has its own distinctive cytokine interstitial pattern with high expression of the interleukin-2 gene, but the possible clinical significance of this requires further clarification.
Laboratory diagnostics
- According to a clinical blood test, in most cases normochromic anemia (chronic inflammation), reactive thrombocytosis and a normal number of leukocytes are detected.
- When examining urine, slight proteinuria is sometimes detected.
- Biochemical and immunological blood tests show: an increase in the concentration of C-reactive protein and/or interleukin-6;
- increased content of α2-globulins, coagulation factor VIII;
- sometimes the activity of AST and alkaline phosphatase increases;
- the concentration of immunoglobulins and complement (including individual fractions - C3, C4, CH50) usually remains within normal limits.
Instrumental diagnostics
Today, among the instrumental methods, duplex ultrasound is the optimal method for diagnosing and monitoring patients with Horton’s arteritis in terms of cost, time and information content of the method. Research used a. temporalis superficialis (trunk and branches) and a. occipitalis.
The sensitivity and specificity of this method according to the literature vary significantly and amount to 17-100% and 61-93%, respectively. It is believed that if the study is performed correctly and the size of the hypoechoic halo is more than 1 mm, the sensitivity and specificity exceed 70% and 90%, respectively.
Indications for ultrasound examination a. temporalis superficialis in persons over 50 years of age are:
- headache + increased ESR;
- headache + “lameness” of the lower jaw;
- headache + pathology of the temporal artery;
- headache + blurred vision;
- fever of unknown origin.
The most characteristic signs of Horton's arteritis according to ultrasound examination of large arteries are:
- hypoechoic halo (halo), visible in both projections; A possible reason for the development of a hypoechoic halo is edema of the vessel wall and/or inflammatory infiltrate.
- stenosis(s) or occlusion.
Positron emission tomography may be necessary to confirm Takayasu-like Horton's arteritis. In one study, when performing positron emission tomography in 13 patients, 7 of them (54%) were found to have increased accumulation of 18-deoxyglucose in the abdominal aorta, which may indicate a high incidence of subclinical aortic lesions.
Computed tomography and magnetic resonance imaging can be used to exclude aortic aneurysms if duplex ultrasound is insufficiently informative. Magnetic resonance imaging in angiography mode can also be used to visualize the superficial temporal and occipital arteries. When the above arteries are inflamed, thickening of the walls can be seen on tomograms (when the images are enlarged), as well as the appearance of a “ring symptom” (the walls of the arteries are clearly outlined), which occurs due to the effect of contrast.
To date, morphological examination of material obtained from a biopsy of the temporal artery is the most reliable method for diagnosing Horton’s arteritis, which is the “gold standard”. Although the connection between the presence of a hypoechoic halo and a greater degree of infiltration of the vascular wall with monocytes has not been confirmed by all authors, it is recommended to perform a biopsy at the site of detection of stenosis/occlusion of the vessel or in the area of the hypoechoic halo. There is evidence that in the absence of ultrasound-detectable changes in the arterial wall, only single monocytes are found in the biopsy material around the vasa vasorum and/or in the outer layers of the adventitia. The minimum length of the vessel section for morphological examination should be 18 mm.
Normal results of morphological examination are also possible in the presence of a typical clinical picture and other signs of Horton’s arteritis. It has been shown that this situation is more often observed when:
- the presence of synovitis of another etiology;
- ESR less than 40 mm/h;
- absence of “lameness” of the lower jaw;
- absence of temporal artery pain.
If the patient has all four signs, then the probability of a negative temporal artery biopsy is 95%.
Temporal artery biopsy is an invasive research method. Possible complications include:
- skin necrosis;
- facial nerve damage;
- post-operative eyebrow sagging;
- stroke due to cessation of colateral blood flow (only in persons with severe stenosis of the internal carotid artery).
Treatment
Treatment Goals
- Increased life expectancy.
- Improving quality of life.
- Achieving remission.
- Reducing the risk of exacerbations and the frequency of hospitalizations.
- Preventing irreversible vision loss.
Indications for hospitalization
- Clarifying the diagnosis, assessing the prognosis and selecting treatment.
- A sharp decrease in visual acuity.
- Suspicion of dissecting aortic aneurysm.
Treatment of patients with Horton's arteritis without the threat of vision loss is recommended to begin with prednisolone or its equivalents at a dose of 40-60 mg/day (0.7 mg/kg). Prescribing low doses of prednisolone (20-30 mg/day) as initial therapy in patients with “low-active” disease does not suppress the activity of the immunopathological process. It should be remembered that prednisolone therapy every other day (alternate day therapy) is ineffective.
If the patient had a history of amaurosis fugax, complete or significant loss of vision in one eye, or early signs of damage to the second eye, the following therapy is recommended: a single intravenous administration of methylprednisolone at a dose of 1000 mg, followed by a transition to oral prednisolone at a dose of 60-80 mg/ days
The hypoechoic halo around the affected vessel, as a rule, disappears 2 weeks after the start of adequate therapy. There are no exact recommendations on how to reduce the dose of prednisolone. In each case, it is necessary to make an individual decision based on the values of ESR and C-reactive protein, interleukin-6.
The average maintenance dose of prednisolone is 7-10 mg/day. In most cases, the duration of treatment is more than 2 years.
Simultaneously with treatment with glucocorticoids, it is necessary to carry out anti-osteoporosis therapy and control blood pressure. Methotrexate may be recommended as a standard adjunctive therapy to corticosteroids in patients suffering from Horton's arteritis.
To date, infliximab has been successfully used in several dozen well-tolerated patients with Horton's arteritis, both to achieve and maintain remission. At the same time, the results of a recently published prospective placebo-controlled study (Hoffman GS et al, 2007) demonstrate the ineffectiveness of infliximab at a dose of 5 mg/kg (infusions 0-2-6-every 8 weeks) both in terms of reducing disease relapses and from the position of reducing the total dose of prednisolone.
For all patients with Horton's arteritis, in the absence of absolute contraindications, it is recommended to prescribe acetylsalicylic acid at a dose of 75-150 mg/day for the prevention of ischemic complications (primarily for the prevention of ischemic retinopathy and non-fatal stroke).
Considering the advanced age of most patients, temporary disability does not pose a significant problem for society. In general, the time frame varies significantly depending on the severity of the condition and can be 30-60 days.
Further management
Monthly complete blood count and C-reactive protein. Every two months, a general urine test, ALT/AST when using methotrexate. It is recommended to perform a chest x-ray and ultrasound of the abdominal aorta annually to exclude the possibility of aneurysm formation in the thoracic or abdominal aorta, respectively.
The mortality rate of patients with GCA due to stroke exceeds 75%. Monitoring antineutrophil cytoplasmic antibodies (ANCA) in ANCA-positive patients predicts relapse of GCA symptoms.
Patient Information
Horton's arteritis is a chronic inflammatory vascular disease. The underlying cause of this disease remains unknown. Heredity plays a certain role in the development of the disease, and the disease is not transmitted to children. This disease cannot be contracted through close contact. Horton's arteritis is not life-threatening, however, it can significantly reduce its quality, primarily due to possible complications on the organ of vision (blindness, sharp deterioration of vision). Treatment with prednisone and acetylsalicylic acid is necessary to reduce the risk of blindness, stroke, heart attack, as well as to improve overall health. Throughout treatment, to determine the activity of the disease, you need to focus not only on your well-being, but also on the results of laboratory tests, and therefore you need to regularly visit your doctor.
Forecast
Horton's arteritis tends to become self-limiting after many months or years of onset. Most patients manage to stop taking glucocorticoids over time. To date, there is no evidence that arteritis reduces life expectancy. At the same time, it must be remembered that Horton's arteritis is significantly associated with an increased incidence of non-fatal cardiovascular complications, which significantly worsens the quality of life. First of all, this concerns visual acuity, because Almost every 6 patients with Horton's arteritis suffer from amaurosis.
Treatment of inflammation of the facial artery
Traditional drug therapy for arteritis is carried out in several directions. It is mandatory to prescribe glucocorticosteroids, in large doses at the initial stage with a gradual reduction. An example of such a drug is Prednisolone, the course of use of which can last for 2 years. This is the only method today with proven effectiveness.
In addition to the main medicine, the doctor has the right to recommend immunosuppressants that suppress inflammation, agents for strengthening and dilating blood vessels, reducing the likelihood of thrombosis. Finally, anticoagulants and antiplatelet agents (Aspirin, Heparin, Curantil) are auxiliary substances to improve the patient's condition.
In rare cases, when the disease is advanced or occurs with complications (for example, due to oncology), surgical intervention is resorted to. In this case, bypass surgery of the affected artery or angioprosthesis is performed.
The effectiveness of treatment is assessed by a general blood test. At the same time, the patient must remember that exacerbations are possible, so if headaches recur, you need to consult a doctor again.
An insidious disease that requires immediate treatment is viral conjunctivitis: symptoms and treatment in adults.
The operation is prescribed when the disease has become advanced
A reliable way to diagnose visual acuity is visometry.
Definition
Horton's disease (temporal arteritis, senile arteritis, giant cell temporal arteritis) is a granulomatous arteritis that occurs in people over 50 years of age and is characterized by a unique clinical picture with obligatory damage to the temporal arteries, selective involvement of the branches of the ophthalmic arteries and a frequent combination with polymyalgia rheumatica.
The incidence of HD, according to epidemiological studies, varies widely: from 0.49 to 15 - 30 per 100 thousand population over the age of 50 years, which is explained by the use of various diagnostic criteria, as well as geographical factors. There is an increase in incidence in northern latitudes. The incidence of HD in the seventh and eighth decades of life is almost 3 times higher than in the sixth.










