05.07.2020
Intraventricular hemorrhage (IVH) is a pathology in which small vessels burst and bleed into the ventricles of the brain of a newborn child.
The ventricles are cavities in the brain that are filled with cerebrospinal fluid (CSF). A person has several of them and they are all connected to each other.
The diagnosis of IVH is quite often made in premature infants, which is due to their physiological characteristics. The shorter the gestational age, the higher the likelihood of hemorrhage.
Hemorrhage does not appear just like that; there must be reasons for this disorder.
Who is at risk?
Brain hemorrhage in newborns can be associated both with damage to the skull itself and with a lack of oxygen.
Prerequisites for DRC:
- Post-maturity or, conversely, under-maturity
. Premature babies are especially susceptible to intracranial hemorrhages, since their immature vessels do not yet have sufficient support in the tissues. In babies born late, the bones harden and the head is unable to adjust during birth. According to statistics, IVH occurs in every fifth premature baby and every tenth post-term baby. - The size of the fetal head does not correspond to the size of the birth canal
. In this case, natural delivery is contraindicated, because it is fraught with injury and hypoxia for the newborn baby. - Difficult pregnancy
(fetal hypoxia, intrauterine infection with various infections). - Difficult (protracted or rapid) labor
, breech presentation. - Incorrect actions of obstetricians during childbirth
.
Based on the above, several risk groups can be identified.
The risk of cerebral hemorrhage in a child increases with:
- prematurity;
- low birth weight (less than 1.5 kg);
- oxygen deficiency (hypoxia);
- child's head injury during childbirth;
- breathing complications during childbirth;
- infections leading to blood clotting disorders.
If the child belongs to at least one of these groups, it is necessary to find out whether he has symptoms of intracranial hemorrhage.
Treatment and prognosis
Neurosurgeons and neonatologists treat children with IVH. Conservative therapy is aimed at restoring the functioning of vital organs and blood counts. If the child did not receive vitamin K at birth, it must be administered. Deficiency of coagulation factors and platelets is compensated by transfusion of plasma components. If breathing stops, artificial ventilation of the lungs is performed, but it is better to arrange it as planned if there is a risk of respiratory disorders.

Drug therapy includes:
- Normalization of blood pressure to prevent sharp decreases or surges that aggravate hypoxia and damage to nervous tissue;
- Oxygen therapy;
- Anticonvulsants;
- Blood clotting control.
To reduce intracranial pressure, the administration of magnesium sulfate intravenously or intramuscularly is indicated; diacarb, furosemide, and veroshpiron are used for full-term children. Anticonvulsant therapy consists of prescribing diazepam and valproic acid drugs. To relieve symptoms of intoxication, infusion therapy is carried out; acidosis (blood acidification) is eliminated by using a solution of sodium bicarbonate intravenously.
In addition to medication, surgical treatment of IVH is carried out: evacuation of blood from the ventricles of the brain through their puncture under ultrasound control, introduction of fibrinolytic agents (actelyse) into the lumen of the ventricles to prevent thrombosis and occlusive hydrocephalus. It is possible to combine puncture with the administration of fibrinolytic drugs.
In order to remove tissue breakdown products and eliminate symptoms of intoxication, liquor filtration, liquor absorption and intraventricular lavage with artificial cerebrospinal fluid preparations are indicated.
In case of blockage of the cerebrospinal fluid ducts and hydrocephalus syndrome, temporary drainage of the ventricles is established with the evacuation of blood and clots until the cerebrospinal fluid is cleared and the obstruction of its outflow tract is eliminated. In some cases, repeated lumbar and ventricular punctures, external ventricular drainage, or temporary internal drainage with implantation of artificial drainage under the skin are used.
insertion of a catheter for ventricular drainage
If hydrocephalus has become persistent and irreversible, and there is no effect from fibrinolytic therapy, then neurosurgeons provide permanent drainage surgically:
- Installation of permanent shunts with the outflow of cerebrospinal fluid into the abdominal cavity (a silicone tube passes under the skin from the head to the abdominal cavity, the shunt can be removed only if the child’s condition has stabilized and hydrocephalus has not progressed);
- Endoscopic anastomosis between the ventricles of the brain and the basal cistern.
The most common method of surgical treatment of occlusive hydrocephalus due to IVH is ventriculoperitoneal drainage. It is affordable, allows drugs to be administered into the ventricles, has a low probability of infection, can be carried out for a long time, and caring for the child is not accompanied by difficulties. The use of alteplase, which accelerates the dissolution of blood clots in the ventricles, can reduce mortality and maximize brain function.
The prognosis for IVH is determined by the stage of the disease, the volume of hemorrhage and the location of brain tissue damage. In the first two degrees of IVH, blood clots resolve on their own or under the influence of treatment, without causing significant neurological disorders, therefore, with minor hemorrhages, the child can develop normally.
Massive intraventricular hemorrhages, especially if they are accompanied by damage to brain tissue, can lead to the death of an infant in a short time, and if the patient survives, it is difficult to avoid neurological deficits and severe disturbances in psychomotor development.
All children with intracranial hemorrhages are subject to careful monitoring in intensive care settings and timely surgical treatment. After installing a permanent shunt, the disability group is determined, and the baby should be regularly shown to a neurologist.
To avoid the severe changes described, it is important to follow measures to prevent brain damage in newborns and very premature infants. Expectant mothers need to undergo the necessary preventive examinations and examinations in a timely manner, and if there is a threat of premature birth, the task of obstetricians and gynecologists is to prolong the pregnancy as much as possible with medications until such a time when the risk of hemorrhages becomes minimal.
If the baby is still born prematurely, he is placed in the intensive care unit for observation and treatment. Modern methods of diagnosing and treating IVH can not only save babies’ lives, but also significantly improve their quality, even if this requires surgery.
Brain hemorrhage in newborns is a serious pathology that develops as a result of damage to the vessels of the dura mater or rupture of a cerebral vessel. This often happens with birth injuries. According to statistics, intracranial hemorrhage (ICH) occurs in 1 in 1000 cases in full-term infants. However, very premature babies born with a body weight of less than 1.5 kg suffer much more often - hemorrhagic cerebral bleeding occurs in 20-45%.
The consequences of cerebral hemorrhage in newborns are always unfavorable, as they are fraught with complications such as neurological pathologies, hydrocephalus, cerebral palsy, cerebral edema, impaired vision, motor activity, speech apparatus, and even death. It all depends on the degree of hemorrhage, its location, the general condition of the baby and the compensatory abilities of the brain.
Possibilities of modern medicine
If a child is found to have hemorrhage in the ventricles of the brain, he should be under the vigilant supervision of medical staff. The baby's condition is monitored to ensure his stability.
Basically, therapy for IVH is aimed at eliminating complications and consequences. If any diseases arise as a result of hemorrhage, appropriate treatment is prescribed.
Sometimes (if too much fluid accumulates in the brain), the following measures are applied:
- Ventricular
(through the fontanel) or (through the lumbar)
puncture
. - when a special drainage tube is inserted into the ventricles. It is pulled under the skin into the patient's abdomen, where excess cerebrospinal fluid is absorbed. The drainage system must remain in the body at all times, and the tube must be replaced if necessary.
It should be noted that for the majority of patients (with degrees 1 and 2 IVH) no therapy is required at all; one can count on a favorable outcome.
Be careful, video of the operation! Click to open
Intraventricular hemorrhage – Charitable Foundation for Premature Babies “Right to a Miracle”
The brain has a very complex structure. In addition to gray and white matter, the brain contains structures filled with a special fluid called cerebrospinal fluid. The internal structures of the brain filled with cerebrospinal fluid are called the ventricles of the brain; there are only four of them: two lateral, a third and a fourth. Liquor is formed in the ventricles of the brain, flows through them, then enters the intrathecal spaces of the brain and spinal cord and is absorbed there into the circulatory system.
Due to the immaturity of the entire brain, premature babies are at risk of rupture of fragile cerebral vessels and the development of hemorrhage in the brain, and most often this hemorrhage occurs in the ventricles of the brain.
Intraventricular hemorrhage (IVH) is bleeding into the ventricles of the brain.
The younger the baby's gestational age, the higher the incidence of IVH. The incidence of IVH is especially high in children born before 28 weeks of gestation. Typically, IVH develops within the first 3 days after birth.
IVH is diagnosed using brain ultrasound (neurosonography - NSG). There are three degrees of IVH.
Stage 1 IVH is a small hemorrhage. If the child’s condition has stabilized and no progression of hemorrhage is observed, then grade 1 IVH becomes harmless; it, as a rule, does not lead to complications and does not require treatment. A child with stage 1 IVH undergoes neurosonography several times to make sure that the hemorrhage does not progress and then enters the resolution stage. IVH of the 1st degree does not have an adverse effect on the development of the child.
IVH of 2 and, especially, 3 degrees are already more significant hemorrhages that can affect both the child’s condition and lead to complications. With IVH of the 2nd degree, there is an outpouring of blood into the ventricle; with IVH of the 3rd degree, hemorrhage also occurs in the brain substance surrounding the ventricle (periventricular region). The development of IVH of degrees 2 and 3 can worsen the general condition of the child, worsen breathing, lead to apnea (stopping breathing) and impaired cardiac function. It is also possible to develop seizures. Treatment is carried out taking into account all developing symptoms.
With massive outflow of blood into the ventricles of the brain, the risk of the main complication— occlusive hydrocephalus— . Unfortunately, there are currently no treatments that can prevent this complication.
Occlusive hydrocephalus (dropsy of the brain) is characterized by progressive expansion of the ventricles of the brain as a result of impaired outflow of cerebrospinal fluid. Blockage of the cerebrospinal fluid outflow tract occurs due to the proliferation of certain cells in the walls of the ventricles under the irritating influence of blood and its breakdown products. Thus, cerebrospinal fluid continues to form in the ventricles of the brain, but since the outflow tract is blocked, the cerebrospinal fluid accumulates more and more in the ventricles, leading to their progressive expansion and increased intracranial pressure. In such cases, neurosurgical assistance is required. At the beginning, ventricular punctures (punctures of the cerebral ventricle) can be performed to remove excess cerebrospinal fluid; temporary drains (tubes for draining cerebrospinal fluid) can also be installed into the cerebral ventricle. When the child’s condition allows, then the main stage of neurosurgical treatment is carried out, which should ensure constant drainage of cerebrospinal fluid from the ventricles.
The prognosis for the development of a child with IVH of degrees 2 and 3 is determined by the degree of damage to the brain substance and the presence of occlusive hydrocephalus. With grade 2 IVH without hydrocephalus, there is a high probability of subsequent favorable development of the child. With IVH of the 3rd degree, as well as if occlusive hydrocephalus develops, the risk of impaired psychomotor development of the child, the formation of cerebral palsy, and epilepsy increases.
Kryuchko Daria Sergeevna
Head of the Department for Analysis and Coordination of Work to Improve the Provision of Neonatological Care
FSBI "Scientific Center of Obstetrics, Gynecology and Perinatology named after Academician V. I. Kulakov of the Ministry of Health of the Russian Federation,
Director of the Directorate of Social Projects of the Foundation for Socio-Cultural Initiatives.
Scientific editor of the journal “Neonatology. News, opinions, training."
Doctor of Medical Sciences.
19.01.2019
Preventive measures
It is impossible to prevent hemorrhage in the baby’s brain one hundred percent, but to reduce the risk, some measures can and should be taken.
Correct determination of delivery tactics
Often perinatal intracranial hemorrhages occur due to birth injuries, so it is extremely important to carefully assess the relationship between the mother’s pelvis and the fetal head.
If there is a discrepancy, natural childbirth is contraindicated and a caesarean section is prescribed. This operation is also performed for diseases associated with a decrease in platelets in the blood of a pregnant woman or fetus (poor clotting).
In addition, in this case, special therapy is prescribed (corticosteroids, immunoglobulin, platelet mass). During childbirth, it is important to monitor the baby's blood pressure; it is necessary to avoid its fluctuations so that cerebral blood flow does not increase.
Prenatal screening
Although these studies are not mandatory for a pregnant woman, they should not be ignored.
In addition, you should know that intracranial hemorrhages are possible not only in newborns. They can occur as a result of injury at absolutely any age.
The birth of a child is a rather unpredictable process and often the baby’s health suffers as a result. Brain damage resulting from and is of particular danger to the baby’s health. Oxygen starvation of the brain can lead to intraventricular hemorrhage (IVH) in newborns. The risk of such a complication lies mainly in children who were born prematurely. This is due to the immaturity of blood vessels and structural features of the brain in this group of newborns. Premature babies have a special structure in the brain - the germinal matrix, the cells of which subsequently create the framework of the brain, migrating to the cortex. Intraventricular hemorrhage in newborns occurs as a result of rupture of the vessels of the germinal matrix and the flow of blood into the lateral ventricles. As a result of IVH, the migration of germinal matrix cells occurs with disturbances, which has a detrimental effect on the development of the child, causing delays.
Degrees of residential housing complex
- IVH stage 1 - hemorrhage is limited to the wall of the ventricles, without spreading to their cavity.
- IVH stage 2 – hemorrhage penetrates into the ventricular cavity.
- IVH stage 3 – disturbances in the circulation of cerebrospinal fluid occur, causing hydrocephalus.
- IVH stage 4 – hemorrhage spreads to the brain tissue.
IVH of grade 1 and 2 in newborns are usually characterized by an asymptomatic course, and they can only be detected through examination with additional methods (computed tomography, neurosonography).
Consequences of IVH
The consequences of IVH for the health of a newborn depend on many factors, in particular the severity of hemorrhage, the gestational age of the baby, the presence of developmental pathologies and concomitant diseases. IVH of the 1st and 2nd degrees in newborns in 90% of cases resolves without a trace, without causing serious harm to the health of the child. IVH grades 3 and 4 cause motor disorders and neuropsychological problems.
The brain has a very complex structure. In addition to gray and white matter, the brain contains structures filled with a special fluid called cerebrospinal fluid. The internal structures of the brain filled with cerebrospinal fluid are called the ventricles of the brain; there are only four of them: two lateral, a third and a fourth. Liquor is formed in the ventricles of the brain, flows through them, then enters the intrathecal spaces of the brain and spinal cord and is absorbed there into the circulatory system.
Due to the immaturity of the entire brain, premature babies are at risk of rupture of fragile cerebral vessels and the development of hemorrhage in the brain, and most often this hemorrhage occurs in the ventricles of the brain.
Intraventricular hemorrhage (IVH)
- This is a hemorrhage into the ventricles of the brain.
The younger the baby's gestational age, the higher the incidence of IVH. The incidence of IVH is especially high in children born before 28 weeks of gestation. Typically, IVH develops within the first 3 days after birth.
IVH is diagnosed using brain ultrasound (neurosonography - NSG). There are three degrees of IVH.
IVHK 1st degree
- This is a slight hemorrhage. If the child’s condition has stabilized and no progression of hemorrhage is observed, then grade 1 IVH becomes harmless; it, as a rule, does not lead to complications and does not require treatment. A child with stage 1 IVH undergoes neurosonography several times to make sure that the hemorrhage does not progress and then enters the resolution stage. IVH of the 1st degree does not have an adverse effect on the development of the child.
IVH 2 and especially 3 degrees
- these are more significant hemorrhages that can affect both the child’s condition and lead to complications. With IVH of the 2nd degree, there is an outpouring of blood into the ventricle; with IVH of the 3rd degree, hemorrhage also occurs in the brain substance surrounding the ventricle (periventricular region). The development of IVH of degrees 2 and 3 can worsen the general condition of the child, worsen breathing, lead to apnea (stopping breathing) and impaired cardiac function. It is also possible to develop seizures. Treatment is carried out taking into account all developing symptoms.
With massive bleeding into the ventricles of the brain, the risk of the main complication— occlusive hydrocephalus—
. Unfortunately, there are currently no treatments that can prevent this complication.
Occlusive hydrocephalus
(dropsy of the brain) is characterized by progressive expansion of the ventricles of the brain as a result of impaired outflow of cerebrospinal fluid. Blockage of the cerebrospinal fluid outflow tract occurs due to the proliferation of certain cells in the walls of the ventricles under the irritating influence of blood and its breakdown products. Thus, cerebrospinal fluid continues to form in the ventricles of the brain, but since the outflow tract is blocked, the cerebrospinal fluid accumulates more and more in the ventricles, leading to their progressive expansion and increased intracranial pressure. In such cases, neurosurgical assistance is required. At the beginning, ventricular punctures (punctures of the cerebral ventricle) can be performed to remove excess cerebrospinal fluid; temporary drains (tubes for draining cerebrospinal fluid) can also be installed into the cerebral ventricle. When the child’s condition allows, then the main stage of neurosurgical treatment is carried out, which should ensure constant drainage of cerebrospinal fluid from the ventricles.
The prognosis for the development of a child with IVH of degrees 2 and 3 is determined by the degree of damage to the brain substance and the presence of occlusive hydrocephalus. With grade 2 IVH without hydrocephalus, there is a high probability of subsequent favorable development of the child. With IVH of the 3rd degree, as well as if occlusive hydrocephalus develops, the risk of impaired psychomotor development of the child, the formation of cerebral palsy, and epilepsy increases.
Kryuchko Daria Sergeevna
Head of the Department for Analysis and Coordination of Work to Improve the Provision of Neonatological Care
FSBI "Scientific Center of Obstetrics, Gynecology and Perinatology named after Academician V. I. Kulakov of the Ministry of Health of the Russian Federation,
Director of the Directorate of Social Projects of the Foundation for Socio-Cultural Initiatives.
Scientific editor of the journal “Neonatology. News, opinions, training."
Doctor of Medical Sciences.
01.05.2010, 07:21
Hello. Please help me cure the child. Extract data from the RD:
Pregnancy: 2 births, 2nd pregnancy, at 39-40 weeks, ACS, clear waters, “boiled” placenta. Pregnancy 1.2 ha - without any features. Apgar score 8-9 points, boy 4070 g, 56 cm, approx. Goal. 35 cm, approx. breasts 37 cm. The child’s condition in the following days: satisfactory. at birth, deterioration by the end of 1 day to moderate severity due to the syndrome of vegetative-visceral disorders, regurgitation (after each feeding in the volume of the mixture eaten). Attached to the breast on the 5th day, the umbilical cord fell off on the 4th day, jaundice: no. MUMT on day 6: 354 g, 8.6% Weight at discharge: 3716 (maximum weight loss) The mother refused further stay in the RD. An examination was carried out: NSG on the 2nd day of the child’s life: In the projection of the caudate nuclei, a hematoma of 1.4-0.5 cm is located supependimally on the left. It has a heterogeneous structure due to small pseudocysts, the stage of lysis, intrauterine hemorrhage cannot be excluded. IVH 1st degree, left. X-ray of the cervical spine: signs of injury in the cervical spine at the level of C3 (dislocation of C3 posteriorly within 1.0 mm) Examination by a surgeon on the second day of life: EGD - acute erymatous reflux esophagitis, acute erosive-hemorrhagic gastritis. Neurologist: Cerebral ischemia of hypoxic origin, vegetative-visceral disorders, regurgitation, 1st degree IVH on the left. Treatment carried out: c. Shantsa, Infusion therapy according to indications for up to 6 days. according to physiological needs. Audiological screening on the 5th day: BP is normal, AC is not. Repeated screening at 1 month is recommended. Clinical analysis: Cerebral ischemia stage 2 of hypoxic origin, IVH stage 1, see vegetative-visceral disorders, regurgitation, o. erythematous reflux esophagitis, o. erosive-hemorrhagic gastritis. Gr. risk for IUI. Health group: 3 Risk factors: 16 b.
Examination by a pediatrician on the 7th day: Breastfeeding, on demand, sufficient lactation. Wakefulness is calm, sleep is calm, with a total duration of up to 20 hours per day, the physique is correct, muscle tone is dystonic, reduced in the arms (more in the proximal parts of the arms) more than in the legs. Reflexes of a newborn: proboscis +, searching +, sucking +, grasping +, support: no 2 phases. Robinson, leg abilities quickly fade, crawling+, automatic gait+. Visual analyzer: 7 days, auditory analyzer: 7 days. The skin has a physiological color, turgor is reduced, subcutaneous tissue is developed moderately and evenly. Musculoskeletal system: no visible deficiencies, short neck (underlined by the pediatrician with a wavy line), “doll’s hand” Fontana: 2.0x2.0 at the level of bone formations, dense skull bones.
Examination by a neurologist on the 25th day: Complaints about changes in the NSG, chin tremor Ob.no: about goal. 38 cm, br 3.0x3.0, not tense. General cerebral symptoms: regurgitation of the IMN - the gaze is fixed, there is no ptosis. Smoothness of the right nasolabial fold. There are no bulbar disorders. Is your hearing reduced on the left? Muscle strength is not reduced. Muscular dystonia with increased tone in the bends of the arms, adductor muscles of the thighs (more on the right). The doll's head, lying on its stomach, does not rest well on its right arm. When verticalizing, rest on the top edge of the feet, tuck the toes, step reflex with the legs crossing at the level of the feet. The reflexes of a newborn are alive. D-z: post-hypoxic-ischemic post-hemorrhagic perinatal encephalopathy, hydrocephalic s-m, syndrome of neuromuscular dystonia, vegetative-visceral disorders. Recommended: 1. EPH with 1% aminophylline solution at SHOP according to Rabner 10 2. gliatilin 1.0 IM N12 3. Actovegin 0.5 IM No. 10 4. glycine 0.1 1/2 tablet. under the tongue 1 month. 5. Repeat NSG after treatment 6. Examination by a neurologist, pediatrician
Examination by a pediatrician at 1 month: height 56.5, weight 5170 (+1100 in 1 month) OB 38.5 (+3.5 cm), chest 40 (+3.0), BR 2.0x2.0 Functional condition: no complaints, satisfactory condition. Satisfied nutrition, the skin is clean, dry on the cheeks and behind the ears. Muscle tone is satisfied. Periodically throws back his head. Reflexes of newborns: grasping, Babkin, Robinson lively symmetrical, Moro phase 1, support on curled toes, stepping, defensive, Bauer, Gallant, Perez - see, VI VPR. Conclusion: RF macrosomia, disharmony. due to the environment breast, NPR 1 gr. D-z: PEP, ChChS, s-m NMD, vegetative-visceral dysfunctions. BP, infant var-t, lok. f-ma, beginning p-d
Parents' comment: the child is 1.5 months old, regurgitation sometimes disappears completely, but now it has become more frequent, occurring after almost every feeding (volume of 0.5 teaspoon-3 tablespoons) with both curdled and watery milk. The stool is normally yellow without mucus. Rarely with green splashes. The stomach is swollen. The child is calm, sleeps all night, feeds 2-3 times at night. During the day, the period of wakefulness increases to 4-6 hours. Burps more often when pushing. The child grunts and rarely cries. He can distinguish his mother's voice, perks up at the sight of a breast, turns his head from side to side behind a toy, smiles when addressed to him. The smile is sometimes asymmetrical, the mouth is slightly curved. In a lying position on his stomach, he holds his head for 15-20 seconds. The child arches while crying; if you carry it vertically, he throws his head back.
Questions: 1. Stage 1 IVH - what does it mean in the future? What are the prognoses taking into account medical history and pregnancy. 2. Is it worth using the medications prescribed by the neurologist? 3. After three electrophoresis procedures, a mast rash appeared (in the area where the electrodes were inserted), treatment was stopped. The rash is going away, but slowly (for a week now). Is it worth continuing EFZ? Thank you!
01.05.2010, 10:56
Such intrauterine hemorrhage does not require any treatment. A hematoma of similar size lyses (dissolves) on its own to form a small cyst. You will not be able to influence this process with medication, especially with the drugs prescribed by the neurologist. This treatment is not necessary. Moreover, in addition to being useless, it can also be harmful to the child. Electrophoresis is also not indicated. Only developmental classes are needed. Children are quite flexible, and in the vast majority of cases such problems go away relatively without leaving a trace.
01.05.2010, 11:40
Thank you very much for your answer. But local doctors, on the contrary, say that the worst thing is the formation of a cyst, and in order to prevent this, such drugs are prescribed. Please advise what to pay attention to in the future, so as not to miss the moment and start treating the child (if necessary). Is it a worrying symptom that a child sometimes falls asleep with his eyes open, i.e. Does he sleep with his eyes open at first, and then fall into deep sleep and close his eyes? And one more thing... Will massage and gymnastics provoke any negative phenomena, because... the neurologist categorically forbade physical procedures, because this, according to her, will provoke negative dynamics.
01.05.2010, 12:34
Such cysts are the result of lysis of hematomas. This is a natural normal recovery process. Nature came up with such a mechanism; there is absolutely nothing scary about it. I repeat once again - it is IMPOSSIBLE to influence him with these drugs. Neither massage nor gymnastics can provoke negative phenomena and negative dynamics. And in general, after such statements, I would run away from this neurologist until the child begins to be treated with something even more extravagant.
22.07.2010, 16:57
First of all, thank you very much, dear doctors, for saving my child from a bunch of meaningless injections.:ax::ax::ax: Indeed, according to the results of the NSG, by the end of the second month only a pseudocyst with a diameter of 1.5 mm was discovered. Everything resolved without Actovegin and gliatilin. We did one course of massage and that was it.
Secondly, there is a question about the current condition of the child.
The child is 4 months old. Grabs toys with both hands, brings his hands in front of him, actively babbles, from 3.5 months. rolls over onto his stomach, distinguishes between relatives. What worries me is what the child started doing quite recently.
Having children is a rather unexpected process, and the child’s health often suffers as a result. Brain defects that form as a result of asphyxia and hypoxia during the period of waiting for a baby pose a particular threat to the child’s well-being. This pathology can cause IVH (intraventricular hemorrhage) to appear in newborns. The threat of such a complication awaits mainly a child born prematurely. The reason is the immaturity of the blood vessels and the distinctive features of the brain structure in this category of newborns.
These babies have a special structure in their brain called the germinal matrix, the cells of which subsequently form the brain frame, migrating to the cortex. Intraventricular hemorrhage in newborns occurs due to rupture of matrix vessels and blood entering the lateral ventricles. Due to IVH, cell migration occurs with disturbances, which negatively affects the development of the baby, initiating its delays. But also, post-term pregnancy is no less dangerous. More on this later.
IVH (intraventricular hemorrhage)
Intraventricular hemorrhages (IVH, PIVC, cerebral hemorrhages, periventricular hemorrhages) are hemorrhages in the ventricles of the brain. In other words, this is something similar to a hemorrhagic stroke, when blood enters certain structures of the central nervous system - the ventricles of the brain (they form cerebrospinal fluid, i.e. cerebrospinal fluid, there are four of them in total - two lateral, as well as a third and fourth) .
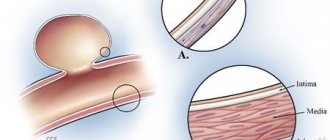
An important role in the development of cerebral hemorrhages in newborns belongs to the anatomical features of the immature body of a premature baby. The greater the degree of prematurity and immaturity, the higher the risk of hemorrhage, especially in children with extremely low and very low body weight (less than 1000 and 1500 grams, respectively). The blood vessels around the ventricles of the brain are very fragile and require very little force to damage and rupture them.
The leading factors in the occurrence of IVH are episodes of hypoxia, as well as traumatic damage to blood vessels (usually due to difficult childbirth). Hypoxia is oxygen starvation, which is accompanied by fluctuations in blood pressure both in general and directly in the vessels of the brain. Hemorrhages are much less commonly associated with primary coagulopathies (blood clotting disorders) or congenital vascular anomalies. IVH also occurs with disseminated intravascular coagulation, isoimmune thrombocytopenia, and vitamin K deficiency.
IVH occurs most often in the first three days of life and can increase in the first week, and much less often occurs after the first week of life.
There are some differences in the classifications of cerebral hemorrhages depending on the location and causes of the hemorrhage; the classification presented below is most often used.
There are four degrees of hemorrhage:
• I degree - a small amount of blood is observed around the vessels. Such subependymal hemorrhage is considered minor and most often disappears on its own without any consequences.
• II degree - blood enters the cavity of the ventricle of the brain, but usually has little effect on the further development of the child, often disappears on its own and without a trace. • III degree - the exit from the ventricles is closed by a blood clot, and the ventricles begin to expand. Some cases are accompanied by spontaneous resolution of the problem, but if this does not happen, surgery is necessary to install a shunt that unblocks the ventricles of the brain, otherwise there is a high risk of developing hydrocephalus. At this degree, manifestations of neurological symptoms are not uncommon.• IV degree - blood enters not only the ventricles of the brain, but also into the surrounding brain tissue - the parenchyma. Such hemorrhage is life-threatening and is accompanied by severe neurological symptoms - most often convulsions, repeated episodes of apnea, the development of anemia, as well as ocular symptoms.
Causes of hemorrhage development.
It is definitely not known why some babies develop hemorrhage and others do not, and what is the immediate cause of brain hemorrhage in premature babies. But the more stable conditions are created for the child, the better, because premature babies require a strict protective regime and stay in a comfortable microenvironment, for which a special incubator is used.
Symptoms of IVH.
Symptoms of hemorrhage may vary. Most often they are absent. However, with extensive hemorrhage, the child’s condition worsens, he becomes agitated, and convulsions and ocular symptoms may occur. The child may be lethargic and less mobile, and muscle tone changes. Anemia develops, and in severe cases, shock and coma. Until the sonographer makes a diagnosis using ultrasound, the clinical picture may be difficult to distinguish from that of a rapidly developing infection.
Treatment of IVH.
Treatment is aimed at eliminating the consequences of hemorrhages and their complications. For example, correction of anemia, anticonvulsant therapy, and for progressive hydrocephalus, a neurosurgical operation is performed - ventriculoperitoneal shunting.
Long-term consequences of hemorrhages.
Minor hemorrhages (grade I), as a rule, do not lead to neurological pathology. Grade II hemorrhages also slightly increase its risk. Data from domestic and foreign studies show that extensive hemorrhages in the ventricles of the brain (III degree) lead to death in approximately 25% of children and a high percentage of disability, while 25% develop progressive expansion of the ventricular cavity, but approximately 50% of children do not experience complications. Of those children who have dilatation of the ventricular cavity, approximately half require surgery to install a shunt. With severe bleeding and hemorrhage into the brain tissue (IV degree), 50-60% of children die. With III and especially IV degrees of hemorrhage, surviving children experience significant impairment of motor functions in the form of cerebral palsy (cerebral palsy), developmental delays, decreased vision and hearing or their complete absence with the development of blindness and deafness. Fortunately, grade III and IV hemorrhages are not that common. It is noted that IVH is more severe in full-term infants than in premature infants.
perihelp.ru
Why does this disease mainly affect only premature babies?
Premature babies have specific structure and periventricular spheres: the arteries in them are in a germinal state and have a simple structure. These arteries are called the “subependymal germinal matrix.” They are very fragile and can easily be injured. Of no small importance is the complication of the decrease of venous blood from these areas, the pathology of the constancy of the internal environment of the body. The impact of concomitant disorders in the blood coagulation system cannot be excluded. It can be both congenital and transient, in other words, temporary (usually due to the influence of certain medications). However, IVH does not occur in all babies born prematurely. For the most part, this also happens when the mother carried the baby. This factor negatively affects the baby's health. And therefore, you need to ensure that there is no post-term pregnancy.
Specific conditions have been identified that contribute to the appearance of IVH in children. Most of them are named below:
- The birth of a completely premature baby.
- Critical moments of hypoxia (lack of air to body tissues).
- High pressure in the venous bed (either during childbirth or during synthetic ventilation).
- Increased blood pressure, which increases brain bleeding.
- Changes in brain blood flow saturation.
- Difficulties of the blood coagulation system.
- Infectious and other inflammatory processes in the mother before childbirth or in children after them.
- Initial resuscitation assistance provided with defects or untimely.
- Regular attacks of respiratory arrest and respiratory pathologies, which are typical for premature and post-term infants.
- Injection into a vein of electrolytes, the concentration of elements in which exceeds their permissible values (this is called hyperosmolarity).
As you can see, there are many causes of IVH in newborns. The parents' task is to eliminate them as much as possible.
What lies behind the letters “IVH” in the diagnosis of premature babies?
When it comes to hemorrhages in newborns, many people associate them with severe traumatic births and medical errors. However, not all hemorrhages are associated with tissue trauma. We will talk about intraventricular hemorrhage (IVH) in newborns. They are typical for children born prematurely and are caused by the physiological characteristics of premature infants. IVH are a very serious problem, because the prognosis for the full life of premature babies largely depends on the nature of the pathological process and its proper treatment.
What are the ventricles of the brain?
To make it easier to understand the origin of IVH and their consequences, it is necessary to know what the ventricles of the brain are. The ventricles of the brain are small cavities that are filled with cerebrospinal fluid. A person has several ventricles connected to each other.
The largest are the paired lateral ventricles, located symmetrically in the brain relative to the midline (one ventricle in each hemisphere). They are connected through small openings to the unpaired third ventricle. The third ventricle is located centrally, it communicates with the cerebral aqueduct. The cerebral aqueduct communicates with the fourth ventricle. This ventricle is formed by the surfaces of the pons and medulla oblongata. It, in turn, communicates with the cerebrospinal fluid spaces surrounding the brain and spinal cord.
Why is liquor needed?
Liquor is a cerebrospinal fluid that is produced in the lateral ventricles of the brain, in their choroid plexuses. The process of liquor production is ongoing. But where does he go? It is continuously absorbed into the venous sinuses located in the dura mater, as well as through the granulations of the arachnoid membrane.
Liquor plays an important role in the human body. The main functions of cerebrospinal fluid:
- Protective role - protects the brain and spinal cord from mechanical influences.
- Maintain intracranial pressure at normal levels.
- Participates in metabolic processes between the blood and the brain (transfer of hormones, electrolytes, etc.), transfers nutrients to nerve cells.
- It is the place where waste products of brain tissue are released.
- It is an immunological barrier to dangerous microorganisms.
What is intraventricular hemorrhage (IVH)?
Intraventricular hemorrhages are hemorrhages in the ventricles of the brain. IVH are typical for children who were born prematurely with very low body weight (less than 1500 g). The shorter the period at which the child was born, the greater the chance that he will develop IVH. Thus, with a gestation period of less than 29 weeks, IVH occurs in almost every third child. When a baby is born at 34-36 weeks, the risk of IVH is significantly lower and is less than 5%.
Why are IVH typical for premature babies?
Premature babies have structural features of the lateral ventricles and periventricular (periventricular) areas. Namely, that the vessels in them are in an embryonic state and have a primitive structure. These vessels are called the subependymal germinal matrix. They are very fragile and can easily be injured.
The difficulty of the outflow of venous blood from the periventricular areas plays a role, as well as a violation of the constancy of the internal environment of the body.
The influence of concomitant problems in the blood coagulation system, which can be both congenital and transient, that is, transient (usually due to the effects of certain medications), cannot be excluded.
But IVH does not occur in all premature babies. Certain factors have been identified that contribute to the occurrence of IVH in a child. Some of them are listed below:
- Birth of a very premature baby;
- Acute episodes of hypoxia (that is, lack of oxygen to body tissues).
- Increased pressure in the venous bed (either during childbirth, or during artificial ventilation);
- Increased blood pressure, which increases cerebral blood flow;
- Fluctuations in the intensity of blood flow to the brain;
- Problems of the blood coagulation system;
- Infectious and other inflammatory processes in the mother before childbirth or in the child after birth.
- Defective or untimely primary resuscitation care in the delivery room.
- Repeated attacks of respiratory arrest (apnea) and breathing disorders that are typical for premature babies.
- Injecting electrolyte solutions into a child’s vein, the concentration of substances in which exceeds their permissible values (this is called hyperosmolarity).
Division of IVHK by degrees
Intraventricular hemorrhages are classified by degree. Some authors distinguish 3 degrees of IVH, others - 4 degrees (dividing the second degree into two).
- In grade I, the hemorrhage is localized in the area of the embryonic vessels, that is, under the ependyma of the ventricles.
- In grade II, hemorrhage breaks through into the ventricular cavity. The ventricle remains the same size or slightly expands.
- In grade III, IVH is also localized in the ventricular cavity, but it expands significantly.
- In grade IV, there is a breakthrough of hemorrhage into the brain tissue.
How to suspect IVH?
- With stage I IVH there are no specific signs; it can be detected during a routine examination of a newborn child.
- The course of stage II-III IVH can be catastrophic and wave-like.
In the catastrophic course of the process, very clear symptoms are noted: suddenly the child becomes excited for a short time, then his activity subsides sharply, consciousness is depressed until coma. Respiratory disorders, changes in skin color, convulsions, eye symptoms, heart rhythm disturbances, drop in blood pressure, and instability of thermoregulation are noted. The undulating course of IVH is characterized by a gradual change in symptoms: changes in phases of brain activity, episodes of respiratory arrest, impaired muscle tone (decrease), and convulsive attacks.
- IVH of stage IV is accompanied by the same symptoms as IVH of stage III, but the process is characterized by a catastrophic course.
There is a disturbance of consciousness up to coma. Additional symptoms appear due to the breakthrough of hemorrhage into the tissue (parenchyma) of the brain. They depend on the size of the hemorrhage and its location. Many children die within the first days of life.
The development of hydrocephalus (dropsy of the brain) is characteristic in many cases after suffering severe IVH. In addition, at the site of hemorrhage in the brain parenchyma, a cystic cavity is subsequently formed, which is filled with cerebrospinal fluid. Depending on the location and size of the cystic cavity, the child will have certain neurological symptoms (eye symptoms, seizures, etc.)
How to confirm the diagnosis?
- The most accessible and very effective method for detecting intraventricular hemorrhages is neurosonography (NSG). In another way, NSG is an ultrasound examination of the brain. It allows you to get results quickly, right at the baby’s incubator. Often in departments where premature babies are cared for, there are small transport ultrasound machines. During the examination, the doctor notes areas of increased echogenicity in the projection of the brain ventricles, which can be on one or both sides and be of different sizes. When performing NSG, it is possible to determine the degree of hemorrhage, assess the size of the ventricles, and the displacement of brain structures relative to the central line.
- Computed tomography (CT), magnetic resonance imaging (MRI) are applicable for the diagnosis of IVH, but these methods do not have advantages over NSG, so their use only for the primary diagnosis of IVH is not advisable.
- Doppler examination of cerebral vessels is of auxiliary value in the diagnosis of IVH; it allows one to evaluate changes in blood flow in the main cerebral arteries before and after a hemorrhage occurs.
- It is very important to constantly measure blood pressure in severely premature infants and evaluate heart rhythm. A sharp drop in blood pressure for no apparent reason may indicate IVH has occurred.
- It is necessary to monitor red blood counts (drop in hemoglobin and hematocrit levels), monitor electrolyte disturbances, and blood gas values.
- Spinal puncture - increased pressure during the flow of cerebrospinal fluid in combination with changes in its other parameters: blood in the cerebrospinal fluid, increased protein levels, decreased sugar levels, pleocytosis (increased number of cells in the cerebrospinal fluid), etc.
All of the above methods for examining a sick child with IVH are carried out repeatedly. This is necessary to assess the dynamics of the process and to identify complications of hemorrhage.
Why does hydrocephalus occur after IVH?
The formation of hydrocephalus after intraventricular hemorrhage is a frequent and serious complication. This can happen with any degree of IVH, but the greater the degree of hemorrhage, the greater the risk of developing the problem.
As IVH resolves, blood clots form, which can clog the already small areas of cerebrospinal fluid outflow from the ventricles. When the outflow is disrupted, cerebrospinal fluid accumulates in the cavity of the ventricle, which leads to its expansion and compression of the surrounding brain tissue. The correct name for this process is posthemorrhagic ventriculomegaly. Ventriculomegaly means the ventricles become enlarged.
In 65% of cases, ventriculomegaly increases slowly, and the process itself spontaneously stops in less than a month. This is the most favorable outcome for a sick child.
In approximately 30% of cases, there is a long-term and slow increase in the size of the ventricles (that is, longer than 1 month). Of these, in every third child the process does not stop spontaneously. In the remaining 67% of children in this group, ventriculomegaly ceases spontaneously. However, in 5% of children, after the ventricles stop increasing in size, the process resumes.
In 5% of cases, the process of enlargement of the ventricles occurs very quickly, which requires urgent surgical intervention.
All these statistics indicate that children who have suffered IVH are observed by specialists for a long time. These include a pediatrician, neurologist, ophthalmologist, and, if necessary, a neurosurgeon and other specialists.
Observation and treatment of children with IVH
Considering that intraventricular hemorrhages are the fate of mainly very premature babies, they are monitored in the neonatal intensive care unit and the nursing department for children born prematurely. The medical and protective regime in the department is very important. Doctors and nurses try to schedule most manipulations at the same time, so as not to disturb the child again. After all, even weighing a very premature baby outside the incubator is very stressful for him and can provoke IVH. The hospital staff takes very careful care of premature babies.
It is necessary to take into account that in addition to IVH, very premature babies have a lot of other associated problems: immaturity of the lungs and difficulties with breathing, cardiovascular disorders, problems with digestion of food, frequent layering of the infectious process, etc. Therefore, the symptoms of a hemorrhage that occurs are “mixed” with signs of related problems. This requires careful monitoring of premature babies, taking a large number of tests and conducting additional research methods.
In premature babies, it is important to monitor head circumference. If it grows by more than 10 mm in 1 week, it is necessary to periodically monitor the size of the ventricles using the NSG method.
As for the treatment of IVH, it depends on the degree of hemorrhage and its complications.
- Carrying out serial spinal punctures. Some specialists use this treatment method for persistent ventriculomegaly in order to “unload” the ventricles. Although there is evidence of the ineffectiveness of such therapy.
- Prescription of medications that reduce intracranial pressure, have anti-edematous and diuretic effects. These drugs only help combat concomitant problems with ventriculomegaly, but do not “cure” it.
- External ventricular drainage. During the operation, the child is fitted with a shunt (tube) connecting the ventricle and a reservoir for cerebrospinal fluid, which is implanted under the skin. This allows you to “dump” excess cerebrospinal fluid from the ventricles. This treatment measure is temporary.
- Installation of a permanent shunt. This operation is usually performed when the child grows up and gets stronger. The shunt is installed as follows: one end goes into the ventricle, the other is brought into the child’s abdominal cavity (most often), where excess cerebrospinal fluid will be discharged. Sometimes complications from the operation occur, such as blockage of the shunt or infection.
Long-term forecasts and consequences
It is difficult to talk about the prognosis and consequences of IVH for children, since many problems of very premature children are explained by other concomitant pathologies. Although there are some statistics about these consequences.
Severe neurological abnormalities, such as convulsive syndrome, cerebral palsy, mental retardation, occur in 5% of cases after IVH of the first degree, in 15% of cases after IVH of the second degree. Every third child suffers from severe neurological problems after stage III IVH, and 90% of children suffer from stage IV IVH. Naturally, less severe neurological consequences after intraventricular hemorrhages are very common.
medaboutme.ru
Degrees of residential housing complex
There are four levels of disease severity. It is worth familiarizing yourself with each of them in more detail:
- IVH of the 1st degree in newborns - the hemorrhage is limited by the wall of the ventricles, without spreading into their recess.
- IVH of the 2nd degree - falls into the recess of the ventricles.
- IVH of the 3rd degree is a pathology in the circulation of cerebrospinal fluid that initiates hydrocephalus.
- IVH stage 4 - hemorrhage spreads to the brain tissue.
IVH of the first and second severity levels in newborns are usually asymptomatic, and they can only be identified through examination with additional methods.
Severity
There are several classifications of hemorrhages, most of them include 4 stages. Below is the gradation most often used in modern medicine:
- IVH of 1st and 2nd degrees. Hemorrhage is observed in the projection of the germinal matrix and does not spread into the lumen of the lateral ventricles. In the second stage, the hemorrhage is slightly larger (1 cm) than in the first.
- At grade 3, hemorrhage from the germinal matrix enters the lumen of the lateral ventricles. As a result, posthemorrhagic ventriculomegaly or hydrocephalus develops. On the tomogram and section, expansion of the ventricles is observed, in which blood elements are clearly visible.
- Grade 4 is the most severe, IVH breaks through into the periventricular parenchyma. Hemorrhage is observed not only in the lateral ventricles, but also in the substance of the brain.
It is possible to establish one or another degree of hemorrhage only with the help of a special study.
The consequences will depend on the degree of IVH and the adequacy of the actions of the medical staff:
- Grades 1 and 2 hemorrhage often do not require any treatment. Such infants need to be monitored; the likelihood that any neurological abnormalities will occur is low. Cases of the development of hydrocephalus and death with 1st and even 2nd degree disorders are extremely rare.
- 3rd degree. When hemorrhage breaks through into the ventricles, the likelihood of developing hydrocephalus increases; it can occur in approximately 55 percent of cases. Neurological abnormalities are observed in 35%. On average, death occurs in every fifth child. Patients are indicated for surgical intervention, and the outcome depends on the extent of brain damage and location (prognosis is more favorable if IVH is present within only one lobe, especially only in the frontal lobe).
- 4th degree. Unfortunately, the prognosis for such severe pathology is disappointing. Surgical intervention in this case is inevitable, but the risks of death remain high - approximately half of infants with stage 4 IVH die. In 80% of cases, hydrocephalus develops, in 90% - neurological abnormalities.
Diagnostics
Medical diagnosis of brain defects, in particular in severely premature infants, is very difficult. This is due to the complete immaturity of organs and tissues, poor health caused by somatic pathology, as well as problems with examination in the incubator and while on artificial ventilation. Mothers who have had a baby are advised to consult a doctor for an examination. After all, the problem may not be visible in the initial stages with the naked eye. Pathology is diagnosed using the methods listed below.
Neurosonography
Neuroimaging is of primary importance in the early diagnosis of IVH and other intracranial defects. The obvious advantages of NSG are safety, speed, non-invasiveness, reliability, financial accessibility, absence of the need for sedation and radiation exposure, and the likelihood of repeated intra-vascular studies. Transfontanel NSG is considered the main method for diagnosing IVH in newborns. In this case, recognition through the large fontanelle is mainly focused on assessing the state of supratentorial structures, including lateral structures and ventricles. More informative recognition is frontal, at the level of the foramina of Monroe; and parasagittal, at the level of the thalamocaudal notch. In order to better visualize the structures of the posterior cranial fossa, additional study through the mastoid fontanel is necessary. With NSG, hyperechoic zones are formed in the matrix area, blood clots in the ventricles and ventriculomegaly can be detected.
Ultrasound and CT
The diagnosis of VJ in babies is established on the basis of anamnesis, general clinical picture, information from transfontanelle ultrasound or CT, and determination of risk conditions associated with weight at birth.
Post-term babies, whose head volume does not correspond to the parameters of the mother's pelvis, are often diagnosed late, at the age of approximately one month, if the gradual accumulation of subdural exudate leads to an increase in head circumference, drooping forehead, protrusion of the large fontanelle, convulsive seizures and anemia. Late manifestation often leads to thoughts of cruel behavior with a newborn.
Subarachnoid hemorrhages often cause short-term convulsions against the background of a relatively mild condition. Although in premature infants intense intraventricular hemorrhages quickly give colorful clinical manifestations: shock, marble-cyanotic skin coloring, anemia, coma, bulging of the large fontanelle, they do not have numerous signs or are not considered characteristic.
Repeated ultrasound scans of the brain in newborns make it possible to recognize later-forming atrophy of the cerebral cortex and porencephaly; talk about the severity, increase or decrease of post-hemorrhagic hydrocephalus. Diffusion-weighted MRI has greatly facilitated early diagnosis and is often prescribed for severe cases.
Prognosis of intracerebral hemorrhage in newborns
In premature infants, intracerebral hemorrhage of grades I-II probably does not significantly increase the risk of neurological complications.
The risk of severe neurological complications in premature infants with grade III hemorrhages is approximately 30%, and with parenchymal hemorrhages - approximately 70%.
In mature neonates, prognosis depends on location and cause; hemorrhages in the basal ganglia, cerebellum and brainstem have an unfavorable prognosis, but the individual course is unpredictable.
The prognosis for subarachnoid hemorrhage is usually good. For subdural, cautious, but some babies do well. Most infants with small intraventricular hemorrhages survive the episode of acute bleeding and appear well. Children with large intraventricular hemorrhage have a poor prognosis, especially if the bleeding continues into the parenchyma. Premature infants with a history of severe intraventricular hemorrhage are at risk of developing posthemorrhagic hydrocephalus and should be closely monitored with repeat cranial ultrasound and frequent repeat head circumference measurements. Infants with progressive hydrocephalus require neurosurgical intervention to place a subcutaneous ventricular reservoir (for CSF aspiration) or a ventriculoperitoneal shunt. The CSF associated with posthemorrhagic hydrocephalus has very low glucose concentrations, known as hypoglycorrachia. Because many children have persistent neurological deficits, close monitoring and referral for early intervention are important.
Observation and treatment of children with IVH
Taking into account the fact that intraventricular hemorrhages are considered to be the lot of premature babies, they are monitored in the neonatal intensive care unit, and then in the nursing department for small children who were born prematurely. It is very important to observe the correct regime in the department. Doctors and nurses strive to schedule most of the manipulations at a constant time, so as not to unnecessarily disturb the children. After all, even measuring the weight of very premature babies outside the walls of the incubator is considered enormous stress for them and can cause IVH. The clinic staff takes very careful care of premature babies.
It should be taken into account that in addition to this pathology, the baby has many other associated problems: immaturity of the lungs and breathing problems, respiratory rate in newborns is disturbed, cardiovascular pathologies, difficulties in absorbing formula or breast milk, frequent layering of the infectious process, etc. For this reason, signs of hemorrhage are mixed with symptoms of other problems. This will require painstaking monitoring of premature babies, taking a significant number of tests and performing additional study methods.
Diagnosis and treatment
The diagnosis is made based on the results of ultrasound examination through the fontanel and computed tomography, as well as based on blood tests.
Treatment of the acute phase is carried out in special conditions while maintaining the desired temperature and ventilation. Therapy is aimed at reducing intracranial pressure and reducing brain swelling. At the same time, it is necessary to maintain cerebral blood flow.
If this treatment does not produce results, surgical intervention is indicated: bypass surgery.
Separately, I would like to say about hemorrhage in the adrenal glands in newborns. In severe cases of hypoxia or improper management of labor, adrenal hemorrhages are possible, which, if not treated in time, lead to death. If such a pathology is detected, treatment is aimed at compensating for adrenal hormone deficiency, increasing blood pressure, anti-shock therapy, restoring water and electrolyte balance and fighting infection, if any.
What are the forecasts?
It is difficult to determine all the consequences of IVH for a child, since numerous difficulties of severely premature children are explained by other concomitant pathologies. It is worth saying that there is still some statistical information about the consequences. Severe neurological differences (convulsions, cerebral palsy, oligophrenia) appear in 7% of cases after IVH of the first degree, in 17% of cases - after the second degree. Every third preschooler suffers from serious neurological difficulties after stage III IVH, and 93% of children suffer from the last stage. Of course, less severe neurological results after intraventricular hemorrhage occur quite often.