Description of the disease
Subarachnoid hemorrhage is a rare cause of stroke when blood leaks from blood vessels along the surface of the brain. Like all strokes, subarachnoid hemorrhage is a medical emergency that requires immediate treatment to prevent serious complications, brain damage, and death.
Subarachnoid hemorrhage is so called because the bleeding occurs in the arteries running under a membrane in the brain called the arachnoid, which lies just below the surface of the skull.
Three quarters of subarachnoid hemorrhages are caused by a ruptured aneurysm. An aneurysm is a bulge in a blood vessel that occurs as a result of weakness in the blood vessel wall.
During a subarachnoid hemorrhage, the blood damages brain tissue. The reduction in blood supply can also cause further damage to the brain, leading to impairment or loss of brain function and possibly death.
How to avoid relapse
It is important to remember that after completing the course of treatment, there is a risk of recurrence of the disease. To avoid new subarachnoid hemorrhages, you must:
- Eat properly. The body must receive all the vitamins and microelements it needs. It is advisable to eat more vegetables and fruits. Avoid fatty and fried foods.
- Avoid bad habits. Alcohol, drugs and nicotine significantly increase the risk of relapse.
- Gradually introduce physical activity. The patient will benefit from jogging, swimming, walking, and regular walks in the fresh air.
- Monitor blood pressure and blood glucose levels. To measure blood pressure, you can purchase a tonometer and carry out the procedure at home.
By following these preventive measures, you can avoid deterioration of the condition and recurrence of hemorrhage. They will also help prevent the development of complications, which in the case of subarachnoid bleeding occur in 80% of patients.
To prevent pathology from leading to irreversible consequences, it is important to seek help at the first manifestations.
Symptoms and signs
Symptoms of subarachnoid hemorrhage include:
- sudden and severe headache - the pain syndrome is described as "a sudden lightning strike to the head" resulting in a blinding pain unlike anything before;
- neck stiffness;
- nausea and vomiting;
- slurred speech;
- changes in personality and behavior such as depression, apathy, or extreme confusion (delirium).
About 30-40% of people with subarachnoid hemorrhage also experience impaired or complete loss of consciousness.
Sometimes the symptoms of a subarachnoid hemorrhage can be similar to meningitis (an infection of the layers of the brain) because in both cases people experience severe headaches and neck stiffness.
Unlike meningitis, people with subarachnoid hemorrhage usually do not have a fever or skin rash. However, both conditions are extremely serious and in either case, you should seek emergency medical attention immediately.
— Warning signs.
About 1 in 10 people will show warning signs that they will have a subarachnoid hemorrhage, usually days or weeks before.
Signs may take the form:
- sudden and severe headache is the most common warning sign;
- dizziness;
- eye pain;
- double vision;
- loss of vision.
If you experience any of these warning signs, it is recommended that you visit your GP, especially if you have not previously had severe headaches.
Parenchymal-subarachnoid hemorrhage
There are mixed forms of hemorrhagic strokes. One of these includes parenchymal-subarachnoid stroke. Its peculiarity lies in its focal symptoms. Depending on the structure affected, specific symptoms will be noted. For example, frontal symptoms with damage to the frontal lobe, visual impairment with damage to the occipital lobe, various types of apraxia and aphasia, impaired coordination and ataxia and other, more severe focal manifestations.
Important! In most cases, these symptoms will persist for life, although they may regress. Prolonged manifestation of focal symptoms is associated with compression or direct destruction of brain structures by the hematoma.
Causes
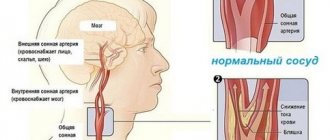
- Blood circulation.
Like all organs in the body, the brain needs blood to provide it with oxygen and other essential nutrients.
Our circulatory system consists of arteries and veins. Blood is pumped from the heart through the aorta (the main artery leading away from the heart) before passing through all the medium and small arteries that branch off from each other. The blood then enters the tiniest vessels known as capillaries, from where the oxygen in the blood is transferred to the cells that make up the tissues and organs of our body.
Capillaries then move the blood into veins, which return it to the heart. Veins are weaker and smaller than arteries, so capillaries must also reduce blood speed and pressure.
Subarachnoid hemorrhages are mainly caused by aneurysms and arteriovenous malformations, which occur due to defects and weaknesses of the blood vessels.
- Aneurysm.
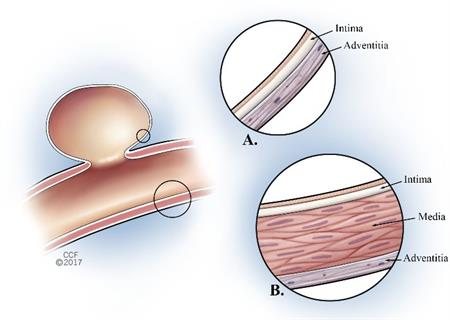
For unknown reasons, approximately 1 in every 100 people are born with defects affecting the blood vessels in their brain. Some of the blood vessels have a thinned and weakened wall that bulges outward like a balloon as blood passes through them. These are known as berry or saccular aneurysms.
When a berry aneurysm ruptures, a subarachnoid cerebral hemorrhage occurs. Not everyone who has this type of aneurysm experiences bleeding. In fact, hemorrhages in people with a saccular aneurysm are very rare, occurring in about 1 in 700 people.
However, a person may increase their risk of aneurysm rupture if:
- smokes;
- drinks alcohol excessively;
- does not control high blood pressure well.
About 70% of subarachnoid hemorrhages are caused by an aneurysm. Once it bursts, the aneurysm often closes and the bleeding stops. However, there is a high risk that without treatment the aneurysm will rupture again and cause more bleeding.
— Arteriovenous malformations.
Arteriovenous malformations occur when blood vessels develop abnormally. They affect approximately 1 in every 100 people and, although the exact cause is unknown, they are thought to be the result of a problem that occurs during the baby's development in the womb.
Arteriovenous malformations can occur anywhere in the body, but they are very rare in the brain, affecting only 1 in every 10,000 people. They can cause problems because they affect the way blood is pumped throughout the body.
Most people with cerebral arteriovenous malformation do not experience any symptoms until bleeding occurs. Arteriovenous malformations cause about one in ten subarachnoid hemorrhages.
- Severe head injury.
Bleeding inside the brain can also occur after a serious head injury.
Why does SAH occur?
The main reason for the outpouring of blood into the subarachnoid space is the damaged integrity of the artery in the skull (its wall) and the subsequent outpouring of blood fluid from it into the subarachnoid zone. The artery is damaged under the following conditions:
- with a traumatic brain injury (this may be a severe bruise of an organ that causes damage to the artery);
- with spontaneous rupture of the arterial wall caused by increased blood pressure, frequent consumption of alcoholic beverages, drugs, and infectious disease;
- when an aneurysm located in the cephalic artery ruptures due to head injury or infection penetration into the brain;
- when an arteriovenous malformation ruptures (a tangle of intertwined veins and arteries formed during the prenatal period, which increases in size during life).
Predisposing sources for the development of pathology include the occurrence of blood diseases, vasculitis, tumor-like neoplasms in any area of the body, fungal pathology, sickle cell anemia, toxic inflammatory process in blood vessels, thrombosis.
Diagnostics
The initial diagnosis of subarachnoid hemorrhage can be made through characteristic symptoms of the condition, such as the sudden onset of a severe headache and a stiff neck.
After the initial diagnosis, it is likely that you will be referred to a specialist neurosurgery unit for further tests to confirm the diagnosis and then decide on the best course of treatment.
The most common tests that are used to investigate cases of subarachnoid hemorrhage are outlined below.
— Computed tomography (CT).
A computed tomography (CT) scan is similar to an X-ray, but it uses multiple scans or images to create a more detailed three-dimensional picture of the brain. The scan can be used to detect the presence and location of blood around the brain and any problems it may cause. Sometimes a colored dye is injected into the blood to help identify the source of the bleeding.
- Lumbar puncture.
The brain and spinal cord are surrounded by a clear fluid called cerebrospinal fluid. If a subarachnoid hemorrhage occurs, there will be blood in the fluid. To obtain a sample of cerebrospinal fluid, a needle is inserted into the lower end of the spine and a sample of the fluid is taken. The procedure may seem painful, but there will be no inconvenience; you will be given a local anesthetic so that you don’t feel anything.
- MRI scan.
Magnetic resonance imaging (MRI) scans use strong magnetic fields and radio waves to produce detailed images of the inside of the body. The scan can be used to identify problems in the blood vessels and, sometimes, to identify the hemorrhage itself.
- Dopplerography.
One of the most serious complications associated with subarachnoid hemorrhage is cerebral vasospasm. This is when the arteries in the brain go into spasm, leading to further blood loss, brain damage and possibly death. Often, cerebral vasospasm does not cause immediate symptoms, so the condition may go unnoticed.
Doppler ultrasound is a test that uses ultrasound to monitor the flow of blood in the brain. Sudden changes in blood flow rate indicate that cerebral vasospasm has occurred, so immediate treatment will begin.
Treatment
Drug treatment
After a subarachnoid hemorrhage occurs, some of the blood vessels near the ruptured aneurysm may go into spasm. This condition is known as cerebral vasospasm, and it can lead to further bleeding, causing brain damage.
To prevent this, the patient may be prescribed a drug called nimodipine (Nimotop) , which must be taken for three weeks. Nimodipine was originally used to treat high blood pressure, but was found to be more useful in preventing cramps. Side effects of nimodipine include:
- increased sweating;
- nausea;
- swelling of the legs, ankles;
- stomach upset.
morphine , can be used to relieve symptoms of severe headaches . paracetamol can be used as an alternative .
Neurosurgical clipping
Neurosurgical clipping is a procedure performed under general anesthesia (when the patient is put to sleep). During the procedure, an incision is made in the scalp and a small piece of bone is then removed to expose the brain.
A neurosurgeon (a specialist in brain and nervous system surgery) will carefully look for the aneurysm and, once located, will close it with a tiny metal clamp. After replacing the “bone flap,” the neurosurgeon will sew the scalp back together.
Neurosurgery is an incredibly complex and difficult procedure, and success can never be guaranteed.
However, neurosurgical clipping has a relatively good success rate, with 70% of people achieving significant or even complete recovery after surgery.
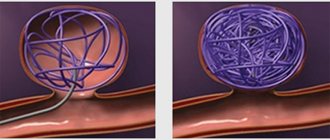
Endovascular coil embolization
Endovascular coil embolization is a procedure in which a tiny plastic tube or catheter is inserted into an artery in the leg or groin. The tube is then guided through a network of blood vessels into the head and finally into the aneurysm.
Tiny platinum coils are then passed through the tube into the aneurysm. These coils block the flow of blood into the aneurysm and thus prevent further bleeding.
Endovascular coil embolization is becoming an increasingly preferred treatment option as it has a higher success rate, with 77% of people achieving significant improvement or complete recovery after surgery.
Additionally, due to the less invasive nature of endovascular coil embolization compared to neurosurgical clipping, recovery time is typically faster.
Rehabilitation
The work of a rehabilitation doctor is successful if the restoration of a stroke brings benefits to the patient, who can live a normal life and take care of himself:
- Move around on your own;
- Bath, eat and clean up after yourself;
- Communicate with people, have interests in life.
The sooner the rehabilitation process begins after a non-traumatic hemorrhagic type of stroke, ischemic type of brain bleeding, or subarachnoid stroke, the greater the chance of restoring all affected body functions.
In this case, time is 50.0% of successful rehabilitation after a stroke. More details about rehabilitation at the link -
Stages of recovery for a patient after surviving an attack of hemorrhage:
- The first stage is an examination of the patient by a doctor and a scheme of rehabilitation steps is prescribed;
- The rehabilitation center has a whole team of specialized doctors;
- The recovery process occurs daily (up to 5 hours a day);
- Medication treatment and physiotherapy are adjusted weekly.
Rehabilitation of a patient after a stroke is designed for 4 calendar weeks with specifically assigned tasks:
- The task for the first calendar week of recovery is to sit the patient up after a long period of lying down;
- The task for the second week is to get back on your feet;
- The goal of the next 14 calendar days is to teach how to move with the help of the necessary means (canes), as well as to learn how to take care of yourself at the everyday level.
Complications
Cerebral vasospasm
Cerebral vasospasm is the most serious complication of subarachnoid hemorrhage and is common. It affects approximately half of people with subarachnoid hemorrhage and is responsible for 20% of deaths or cases of severe brain damage associated with subarachnoid hemorrhage.
However, the incidence of cerebral vasospasm is expected to decrease due to the use of nimodipine as a prophylactic drug.
During cerebral vasospasm, the arteries in the brain go into spasm, cutting off the blood supply to the brain. The causes of cerebral vasospasm are still unknown.
Cerebral vasospasm usually develops three to four days after subarachnoid hemorrhage.
The main symptom is increasing mental impairment. If left untreated, a person may become unconscious, then comatose, and then die.
Brain spasms can be treated with what is called “triple G therapy,” where three Gs mean:
- hypervolemia - which means fluid is pumped into the blood
- hypertension - use of medications to increase blood pressure
- Hemodilution is when extra blood and plasma (the fluid that makes up most of the blood) is transfused into the blood.
The goal of Triple G Therapy is to increase blood flow so the blood supply to the brain is restored.
If triple G therapy is not effective, surgery is usually required to prevent further brain damage. Surgery usually involves implanting a small balloon into the artery and then inflating it to restore blood supply.
Epilepsy
About 5% of people with subarachnoid hemorrhage develop epilepsy.
Epilepsy is a condition in which the normal functioning of the brain is disrupted, leading to repeated seizures or fits (convulsions) in a person.
There are different types of seizures and symptoms may vary. The person may lose consciousness, have muscle contractions (arms and legs may twitch and twitch), or the body may shake or become stiff. The attacks usually last from a few seconds to several minutes. Brain activity then returns to normal.
In most cases of epilepsy following subarachnoid hemorrhage, the first seizure occurs within the first year after the hemorrhage. If more than two years have passed since the bleeding and you have not had a seizure, it is extremely unlikely that you will develop epilepsy.
Epilepsy can be treated with antiepileptic drugs such as phenytoin or carbamazepine. You may need to take these medications for several months or for the rest of your life.
Hydrocephalus
Hydrocephalus is a condition that occurs when too much cerebrospinal fluid forms in the ventricles (cavities) of the brain. About every tenth person suffering from subarachnoid hemorrhage develops hydrocephalus.
Cerebrospinal fluid is produced in the brain and protects the brain and spinal cord by carrying waste away from brain cells. It flows continuously through the ventricles (cavities or chambers inside the brain) and along the surface of the brain and spinal cord. Any excess of this fluid is usually cleared from the brain and absorbed by the body.
Damage caused by subarachnoid hemorrhage can stop fluid from draining and cause excess fluid to accumulate. Symptoms include headache, nausea, vomiting and loss of balance. However, this condition can be treated by placing a tube in the brain to allow fluid to drain properly.
Forecast
Subarachnoid hemorrhage is an extremely serious condition and many people have a poor prospect of survival. 10-15% of people with subarachnoid hemorrhage will die before being hospitalized, and 50% will die within 30 days of the hemorrhage.
However, the prospects for recovery are good if the patient survives the initial bleeding and is quickly transferred to a specialized neurosurgery unit (a medical unit that specializes in treating diseases of the brain and nervous system).
A number of surgical methods have been successfully used in the treatment of subarachnoid bleeding. After treatment, a long period of rehabilitation will be required.