MedStroke -> Types ->
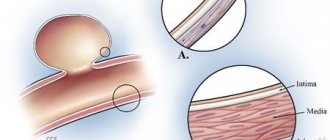
In a healthy person, the blood vessels are usually quite strong and elastic. However, with high pressure, and, therefore, with increased load on the walls of blood vessels, they thin out and become quite fragile. The vessels may not be able to withstand the next hypertensive crisis - they may become clogged or rupture. And the result is a cerebral stroke. If cerebral circulation is disrupted in the brainstem, a brainstem stroke occurs.
- Mechanism of brainstem stroke
- Ischemic brainstem stroke
- Symptoms of a brainstem stroke
- Prognosis for rehabilitation for stroke
Anatomical departments
Anatomically, the brain is divided into the following sections:
- cerebral hemispheres;
- diencephalon;
- midbrain;
- hindbrain;
- medulla.
The brain stem includes all parts except the cerebral hemispheres.
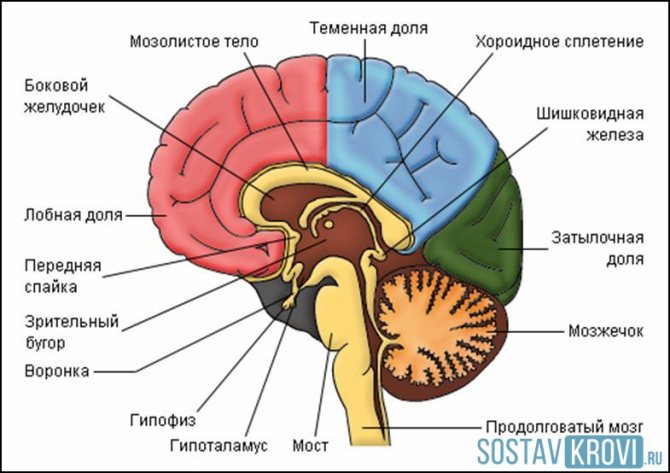
Brain structure
Functions of the brainstem:
- thanks to the sections included in its composition, complex reflexes are formed, which involve the sequential contraction and relaxation of various muscles, for example, the swallowing reflex;
- the brain stem communicates between the spinal cord and the cerebral hemispheres using the nerve pathways passing through it;
- ensures the interaction of various parts of the central nervous system with each other.
The presence of breathing and heartbeat centers in the medulla oblongata indicates the importance of the brain stem.
Alternating syndromes
A brainstem stroke differs from a lesion of the cortex in that the pathological process affects the nuclei and adductor tracts of the motor nerves. The patient suffers from central paralysis and its peripheral manifestations.
Alternating syndromes are sets of symptoms that occur when certain pathways and nuclei are damaged. There are several of them:
- Miillard-Gübler . Paralysis of the facial nerve occurs, in which the corner of the mouth and eyelids droop.
- Jackson. The lesion is located on the side of the medulla oblongata. The swallowing function is impaired, and paralysis of one half of the tongue develops.
- Brissot-Sicara . Caused by an irritating effect on the nuclei of the facial nerve and pyramidal tract. Spastic contractions appear on the affected side.
- Avellisa . Occurs due to thrombosis of the branches of the vertebral artery. There is paralysis of the soft palate and vocal cords, as well as partially of the larynx. In this case, food in liquid form flows into the nose, the person cannot speak normally, and there is a violation of swallowing (he chokes while eating).
- Wallenberg-Zakharchenko . There is a loss of motor function and sensitivity of the facial skin on the opposite side.
Acute circulatory disorders often lead to locked-in syndrome. The patient cannot move, but his intellectual abilities are completely preserved. Therefore, he is able to take an active part in the recovery process.
Types of strokes
According to the development of pathological disorders, all strokes are usually divided into types:
- ischemic strokes , developing due to a disruption in the flow of blood to a certain area of the brain due to blockage of a vessel. Lack of nutrition leads to ischemia - oxygen starvation. If the blood stops flowing or its quantity is critically small, then necrosis of the brain tissue occurs, i.e. its destruction. With ischemic stroke, clinical symptoms develop slowly and gradually increase. It is characterized by: previously identified signs of circulatory disorders in the myocardium, for example, angina pectoris;
- development of stroke after sleep, a hot bath, against the background of an attack of arrhythmia, acute myocardial infarction;
- age over 50 years;
- focal symptoms are brighter than cerebral symptoms.
- development against the background of prolonged arterial hypertension;
If, against the background of cardiovascular pathology, signs of damage to the central nervous system develop, lasting no longer than 24 hours and ending with complete restoration of functions, then they speak of temporary disorders.
These violations are of two types:
- transient ischemic attack (TIA) , characterized by the occurrence of focal brain symptoms, for example, disturbances in movement, swallowing, and speech.
- hypertensive crisis , accompanied by general cerebral symptoms and occurring against the background of sharply increased blood pressure, for example, impaired consciousness, headache, convulsions, vomiting.
Types of brain strokes
Consequences of ischemic cerebral stroke
DlyaSerdca → Cerebral hemorrhage → What to fear after an ischemic stroke?
Ischemic stroke is the most common type, accounting for 80% of all cases of acute cerebrovascular accident. When it occurs, blockage of blood vessels in the brain occurs due to a blood clot, atherosclerotic plaque, or a sharp spasm.
Blood can no longer freely deliver nutrients and oxygen to the affected brain tissue, and the gradual death of gray matter cells begins.
The causes of ischemic stroke lie in:
- Lifestyle. Smoking, physical inactivity, excess weight, addiction to alcohol;
- Age. Starting at age 55, the risk doubles every 10 years;
- The presence of chronic diseases. Diabetes mellitus, congenital or acquired pathologies of the circulatory system, hypertension, atherosclerosis;
- Stress factors. They, in fact, trigger the stroke mechanism.
The consequences of ischemic stroke differ in the degree of reversibility and severity depending on what subtype was diagnosed, how old the victim is and what concomitant pathologies or diseases he has.
According to pathogenesis, ischemic cerebral stroke is divided into the following types:
- Atherothrombotic. Acute pathology of cerebral circulation occurs due to blockage of the lumen of the vessel by an atherosclerotic plaque, against the background of arterial hypertension, the size of the damage can be any (about 30-35% of cases);
- Cardioembolic. A cerebral vessel is blocked by an embolus (an embolus is a particle that under normal conditions should not be in the bloodstream) of cardiac origin due to atrial fibrillation, heart valve disease, chronic heart failure or acute cardiac infarction (about 20% of cases);
- Hemodynamic. Due to a sharp decrease in blood pressure, a narrowing of the lumen of blood vessels occurs against the background of hypotension of various origins, cardiovascular pathology (about 15% of cases);
- Lacunar. Small vessels of the brain are affected, resulting in the formation of lesions up to 1.5 cm in size (lacunae), which occurs against the background of stress and increased blood pressure (about 20% of cases);
- Stroke type of hemorheological microocclusion. Cerebrovascular insufficiency occurs due to changes in blood characteristics (about 5-10% of cases).
Brainstem ischemic stroke
The brain stem connects the brain to the spinal cord. Its length is no more than 10 cm, but it is extremely important: the medulla oblongata, which is part of it, regulates respiratory and cardiac activity, swallowing and thermoregulation.
Even the slightest interruption in blood supply can lead to irreversible consequences, including the death of the victim (if the respiratory or cardiac center is affected). Death occurs in 65-75% of cases.
With a brainstem stroke, blood flow in the arteries passing through the brainstem is disrupted. The most common causes of brainstem stroke are the same as regular ones: atherosclerosis, hypertension, diabetes mellitus, cardiovascular pathologies.
With a brainstem stroke, a situation may arise when the victim’s intellectual abilities are not impaired, but paralysis occurs - this is the so-called “locked-in person” syndrome - the patient understands everything, but can hardly speak or move.
With the brainstem type, it is the motor functions that are most difficult to restore, while classes with a speech therapist can improve speech, and with the help of special therapy, the patient can be taught to eat soft or liquid food (with a brainstem stroke, swallowing function is often affected).
Common Consequences
An ischemic stroke of the brain always causes certain consequences; only 7-10% of victims manage to fully recover from it - with timely help, a small lesion and properly selected therapy.
Most often, after a stroke, hemiparesis is diagnosed - weakening of muscles on one half of the body (85% of cases), motor disorders (70-80% of cases), speech problems: dysarthria and aphasia (30-55% of cases), dysphagia - difficulty swallowing ( 15-25%) and mental disorders - mainly depression (40% of cases).
Paralysis and motor impairment are the most common consequences. Usually one half of the body is affected, depending on which hemisphere of the brain the stroke was localized in: if in the right, then the left side suffers, if in the left, the right. Coordination and motor skills are affected when the source of the stroke is in the cerebellum.
Paresthesia (feelings of numbness and tingling) and peripheral neuropathy (impaired sensitivity) are other frequent companions of the post-stroke period. These two problems can either go away over time (if the stroke was minor and treatment was prescribed in a timely and adequate manner) or turn out to be irreversible.
Cognitive impairment occurs to varying degrees in almost everyone who has suffered a stroke: from slight absent-mindedness to serious problems with memory, understanding, recognition of faces and places, difficulty with orientation in space and time.
Difficulties in everyday life occur in about half of victims of cerebral stroke. The most difficult things are caused by such simple actions as taking a bath and hygiene procedures (45%), eating (35%), dressing independently (30%). About 15% of stroke victims cannot move on their own.
The consequences of repeated ischemic cerebral stroke are more severe and the mortality rate is higher.
Consequences of brainstem stroke
The consequences of a brainstem stroke are divided into:
- Respiratory: rhythm disorder, decreased frequency and depth of breathing, up to the inability to breathe independently;
- Cardiac: interruptions in pulse rate - too rare (bradycardia) or frequent (tachycardia), tachyapnea;
- Motor: lack of control, spontaneity of movements, reduced mobility;
- Vestibular: difficulties with coordination of movements, nausea and dizziness;
- Thermoregulatory: the body loses the ability to adequately regulate its own temperature;
- Visual: impaired oculomotor function leads to strabismus and difficulty focusing vision.
It is especially worth highlighting bulbar syndrome, since it is the “calling card” of a brainstem stroke. When cells in the medulla oblongata are damaged, so-called bulbar palsy can occur.
It manifests itself in dysarthria (impaired speech due to damage to the nerves responsible for speech function: speech becomes quiet, slurred, up to complete aphonia) and dysphagia (impaired swallowing function due to damage to the muscles and nerves responsible for swallowing).
With dysarthria, speech slows down, sounds are distorted and difficult to distinguish, and the patient’s voice changes: it becomes quiet, dull, and sometimes nasal.
Dysphagia occurs due to paresis or atrophy of the muscles that are involved in the swallowing process.
The patient loses the ability to independently eat the usual food; moreover, even liquid or pureed food can cause difficulties and the risk of choking.
Dysphagia is divided into several types: from mild (when it is difficult to swallow only solid food) to severe (when even liquid and saliva are impossible to swallow.
Rarely does complete dysphagia occur, when the swallowing reflex is completely absent. In severe and complete dysphagia, nutrition is only possible parenterally (nutrients are administered into a vein) or nasogastrically (nutrition is supplied through a special tube).
Causes
Due to the fact that there are many reasons for the development of brain stem stroke, they can be divided into local and systemic.
Local causes of stroke:
- structural changes in the brachiocephalic or cerebral arteries;
- atherosclerotic damage to the cerebral arteries;
- varicose veins, atrial fibrillation, aortic aneurysm and heart lesions as a source of thromboebolic infarctions;
- arteritis;
- abnormalities in the structure of blood vessels;
- changes in the cervical spine.
Systemic causes of ischemic and hemorrhagic stroke:
- hemodynamic disturbance;
- violation of the coagulation system;
- blood leukemia.
Risk factors
Research shows that every second cerebral hemorrhage occurs against the background of arterial hypertension, therefore the main and most significant risk factor for hemorrhagic stroke is high blood pressure.
- modifiable , that is, those that can be influenced: arterial hypertension;
- cardiac pathology;
- atrial fibrillation;
- dyslipidemia, or a disorder of fat metabolism;
- diabetes;
- floor;
- smoking;
Symptoms
The following periods of the disease are distinguished:
- acute – up to three days from the beginning;
- acute – up to 28 days;
- early recovery period – up to six months;
- late recovery period – up to 2 years;
- period of residual phenomena - after a two-year period.
Localization of stroke symptoms in the brain stem indicates a severe course of the disease:
- The first significant changes may be disturbances in speech, swallowing, and severe dizziness.
- Dizziness is often accompanied by nystagmus - involuntary frequent movement of the eyeballs in one plane.
- Due to damage to the thermoregulation center, there is an increase or decrease in body temperature.
Due to damage to the vasomotor center, constant rises or very low pressure occur, as well as redness of the skin due to vasodilation or severe pallor due to their narrowing.
Since a structural disruption of the nerve pathways can occur, motor disturbances in the arms and legs occur, up to and including paralysis of the entire body. Coordination disturbances that arise suddenly against the background of complete well-being are also characteristic, for example, an unsteady gait, awkwardness.
If a person suddenly falls sharply, but does not lose consciousness, this may be a sign of the onset of paralysis of all limbs.
When a swallowing disorder develops, a person is unable to swallow not only solid but also liquid food. Because of this, there is a risk of choking and the development of aspiration pneumonia due to food entering the respiratory tract.
With the development of extensive brain damage, when the pathology spreads to the center of breathing or heartbeat, breathing or cardiac activity stops, respectively.
The occurrence of any of the above symptoms requires an emergency medical examination and treatment in a hospital setting. An exception is a refusal of hospitalization signed by the patient or his relative. Then treatment must be carried out at home.
With the development of a hemorrhagic stroke of the brain stem, the most dangerous period is the first day, this is associated with a high probability of recurrent hemorrhage.
For ischemic stroke, experts consider days 3, 7 and 10 to be the most dangerous.
Symptoms of stroke recognition
Possible consequences
More than half of stroke cases end in the death of the victim; in other cases, the patient is doomed to disability.
Subsequently, after a stroke, the following complications may occur:
- slurred, incoherent speech if the speech center in the brain is affected;
- loss of ability to swallow food;
- paralysis of the limbs, inability to walk, sit, or chaotic involuntary movements of the arms and legs;
- pneumonia;
- vein thrombosis;
- internal bleeding;
- myocardial infarction;
- bedsores in bedridden patients;
- mental disorders.
The occurrence of a repeated episode of stroke is especially dangerous; the patient’s body will no longer cope with such a load, and the result will be death.
Treatment
Brain stem strokes are treated in the same way as strokes of other locations. Therapy can be divided into basic and specific.
Basic therapy:
- if consciousness is impaired, then it is necessary to check the airway for patency;
- pressure greater than 170/100 mm Hg requires gradual reduction;
- establish intravenous therapy to normalize the electrolyte composition of the blood;
- to prevent cerebral edema, it is necessary to ensure that the patient is positioned on the bed with the head end raised;
- administration of drugs to prevent increased intracranial pressure and reduce signs of cerebral edema, for example, Mannitol;
- if seizures occur, anticonvulsants are administered, for example, Diazepam;
Specific therapy:
This stroke therapy involves the early introduction of neuroprotective drugs, for example, Cytoflavin, Cortexin, Cerebrolysin.
The earliest possible detection of stroke and transportation of the patient to the hospital makes it possible to treat ischemic stroke using thrombolysis.
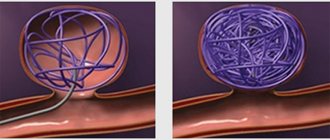
Disintegration of a blood clot during thrombolysis
Researchers believe that when a vessel is blocked by a blood clot, the cells located in close proximity to the affected vessel die in the first hours of the disease. But the zone of impaired nutrition is larger, so cells located further from the vessel, but experiencing ischemia, can recover if blood flow is resumed.
Restoration of blood flow occurs due to the dissolution of the blood clot with special drugs. This is thrombolysis, or thrombolytic therapy.
However, to carry out this procedure there are certain requirements, for example, the duration of the disease is no more than 2 hours, the patient must be conscious. Therefore, it is necessary to detect the disease as early as possible, then the survival rate of patients increases.
Forecast
A brain stem stroke in an adult is severe and can result in disability or death. The prognosis depends on the extent of the affected area of the brain and the timeliness of adequate treatment.
Disability is a common prognosis for cerebral stroke.
Is recovery possible for a brain stem stroke? If we consider recovery as the restoration of all functions of the body and a return to the state that was before the stroke, then no, it is impossible to recover. And if we consider recovery as stabilization of the condition and adaptation to changed conditions of existence, that is, disability, then yes, it is possible.
Recovery prognosis
If the brain stem is affected, the prognosis is poor in most cases. However, if the patient survives, it will be possible to determine the consequences of the disease only after a few days.
In the presence of severe bulbar disorders, recovery is almost impossible. Life in this case is supported by an artificial respiration apparatus. However, if the vital centers have been stabilized, then further rehabilitation depends on the type of complications.
If a brainstem stroke occurs with particularly complex consequences, the patient becomes dependent on special equipment that ensures his vital functions for the rest of his life.
After eliminating life-threatening symptoms, it is imperative to carry out rehabilitation measures. They should start almost immediately.
Initially, therapy includes passive exercise and massage to prevent bedsores and muscle atrophy. As motor functions resume, the patient will be able to perform some exercises independently.
Rehabilitation lasts for the rest of the victim’s life. Any physical or emotional stress or stress is already contraindicated for him. The patient requires proper nutrition, taking into account swallowing disorders.
Prevention
Primary prevention of brainstem stroke involves identifying and eliminating modifiable risk factors. To do this, stroke screening is carried out - a series of examinations aimed at identifying factors.
These include:
- timely detection of arterial hypertension and its correction;
- diagnosis of dyslipidemia and normalization of fat metabolism;
- determination of blood glucose levels;
- ECG and Echo-CG;
- examination of the brachiocephalic arteries using ultrasound;
- performing surgical operations for stenosis of the carotid arteries.
Secondary prevention of strokes is the prevention of the development of various types of stroke complications:
- prevention of contractures, i.e. persistent muscle tension, which leads to the same type of limb position. This complication is associated with prolonged immobility.
- preventing the formation of thrombosis of the veins of the legs and pulmonary embolism using passive exercises, elevated position of the legs and the use of elastic bandaging.
- Prevention of bedsores is ensured by adequate care of the patient’s body, massage, and the use of anti-bedsore mattresses.
- prevention of the development of congestive pneumonia.
What is a brainstem stroke?
This type of stroke affects the brain stem.
It affects the most significant areas of the central nervous system, therefore it is considered one of the most dangerous diseases. It is characterized by high mortality, although there is still a possibility of returning to normal life. It all depends on timely medical care and the extent of the lesion.
Trunk stroke, depending on the nature of the damage, can be:
- Ischemic. Characterized by the formation of foci of necrosis.
- Hemorrhagic. This is when hemorrhage occurs when blood vessels in the brain rupture. The mortality rate is higher in the presence of hematomas.
- Mixed. This type is rare and is a combination of two previous strokes.
The trunk is the connecting link through which “commands” are transmitted from the brain to the spinal cord. A stroke in this location affects the following areas: cerebellum, thalamic region, varoli, medial and medulla pons.
The nuclei of the cranial nerves responsible for a complex of important functions are affected: eye movements, facial muscles, muscles in general, swallowing movements, breathing, thermoregulation and blood circulation.
The resulting hemorrhage and hematoma block the access of oxygen to the affected part of the brain. Over time, this area atrophies, which leads to malfunctions of other internal organs. One such disorder is dysphagia (swallowing function). The person is deprived of the opportunity to eat and has to switch to intravenous nutrition.
People who have suffered from this disease cannot move without assistance. They are worried about frequent dizziness and disorientation in space. Another problem is dysarthria - a disruption in speech function, sometimes accompanied by the inability to swallow food. This syndrome is called bulbar and occurs in 50% of cases.
Rehabilitation
Depending on the severity of the patient’s condition, rehabilitation after a stroke must begin in the intensive care unit. The further prognosis depends on this: the degree and speed of restoration of motor and other functions of the body.
Necessary rehabilitation measures should not be interrupted, that is, when the patient is transferred to the stroke department and then to outpatient treatment, it is important to continue rehabilitation:
- The duration and intensity of rehabilitation exercises should be gradually increased.
- Activities that the patient can perform correctly independently or with the help of relatives are advisable to perform at home.
- To restore speech skills, classes are conducted with a speech therapist.
- Visiting a psychotherapist to stabilize your emotional state.
- Occupational therapy for better social adaptation of patients.