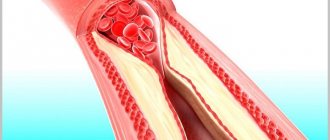
(Seldinger catheterization) is used to gain safe access to blood vessels and other hollow organs. It is used for angiography, catheterization of central veins (subclavian, internal jugular, femoral) or arterial catheterization, gastrostomy placement using the percutaneous endoscopic gastrostomy method of some conicostomy techniques, placement of artificial pacemaker electrodes and cardioverter defibrillators, and other interventional medical procedures.
History of invention
The method was proposed by Sven Ivar Seldinger (1921 - 1998), a Swedish radiologist and inventor in the field of angiography.
Angiographic examinations are based on a technique in which a catheter is inserted into the vessel using a needle for dosed administration of a contrast agent. The problem was that, on the one hand, it was necessary to deliver the substance to the required place, but at the same time minimally damage the vessels, especially at the site of study. Before the invention of Sven Seldinger, two techniques were used: a catheter on a needle and a catheter through a needle. In the first case, the catheter may be damaged when passing through tissue. In the second case, a larger needle is required, which causes much more damage to the vessel at the catheterization site. Sven Seldinger, born into a family of mechanics, tried to find a way to improve angiographic technique by placing the largest catheter with the smallest needle. The technique essentially means that a needle is first installed, a guidewire is inserted through it, then the needle is removed and the catheter is inserted over the guidewire. Thus, the hole is no larger than the catheter itself. The results were presented at a conference in Helsinki in June 1952, and Seldinger subsequently published these results.
The Seldinger method has reduced the number of complications with angiography, which has contributed to the increased prevalence of the latter. This also meant that the catheter could be more easily oriented to the desired location in the body. The invention laid the foundation for the subsequent development of interventional radiology.
Classification of catheterization methods
At the moment, there are at least three catheterization techniques:
- catheter on a needle;
- catheter ears;
- Seldinger catheterization;
“Catheter on a needle” technique
widely used for catheterization of peripheral vessels. Currently, many different peripheral venous catheters have been developed. The vessel is punctured with a needle with a catheter on it, the needle is held in one position, and the catheter is advanced. The needle is completely removed. When used for puncture of deeply located organs (in particular, central veins), the catheter may be damaged when passing through the tissue.
The catheter-in-a-needle technique is used
for catheterization of the epidural space during epidural anesthesia (surgical interventions) and analgesia (childbirth, acute pancreatitis, certain cases of intestinal obstruction, pain relief in the postoperative period and cancer patients), for prolonged spinal anesthesia. It consists in the fact that first the organ is punctured with a needle, and a catheter is inserted inside it. The needle is later removed. In this case, the needle is significantly thicker than the catheter. If large diameter catheters are used, tissue injury occurs when using this technique.
Actually Catheterization according to Seldinger.
Method technique
Seldinger catheterization
proceed in the following order:
- a. The organ is punctured with a needle.
- b. A flexible metal or plastic conductor is inserted into the needle and advanced further into the organ.
- c. The needle is removed.
- d. A catheter is placed over the guidewire. The catheter is advanced along the guide into the organ.
- e. The conductor is removed.
- Figure 3 Removing the needle
Figure 4 Catheter insertion
Figure 5 Removing a conductor
The thinner the needle, the less tissue damage. If the catheter is significantly thicker than the needle, before putting it on the guidewire, an expander is passed along the guidewire, which increases the diameter of the passage in the tissues. The dilator is removed, and then the catheter itself is inserted through the guidewire.
- Figure 1 organ puncture with a needle
Figure 2 Inserting the guidewire into the needle
Figure 3 Removing the needle
Figure 4 Using the expander
Figure 5 Catheter insertion
Figure 6 Removing a conductor
The dilator is especially often used when installing central venous catheters with several lumens. Each lumen of the catheter ends with a port for drug administration. One of the lumens begins at the tip of the catheter (usually its port is marked in red), and the other / other sides (usually its port is marked in blue or another color other than red). Double-lumen catheters are used for administering various drugs (to prevent their mixing as much as possible) and for carrying out extracorporeal therapy methods (for example, hemodialysis).
Possible complications
Depending on the conditions, Seldinger catheterization can be performed either without additional imaging methods or under ultrasound or radiological control. In any case, the following complications may develop with varying frequency:
- Damage to the wall of the corresponding organ by a needle, guidewire, dilator or catheter.
- Damage to surrounding structures by a needle, guidewire, dilator or catheter (depending on the site of catheterization, these can be arteries, nerves, lungs, lymphatic ducts, etc.) with the subsequent development of corresponding complications.
- Inserting a catheter beyond the desired organ and then injecting the appropriate substance there.
- Infectious complications.
- Loss of parts of a damaged guidewire or catheter in an organ, for example. parts of the central venous catheter.
- Other complications caused by the long stay of catheters in vessels and organs.
For central venous access, the right internal jugular vein or the right subclavian vein is most often used. This is due to the fact that the thoracic lymphatic duct passes on the left and can be damaged during catheterization. And also through the internal left jugular vein there is an outflow of blood from the dominant hemisphere of the brain. And in the event of purulent or thrombotic complications, the neurological consequences for the patient may be more serious.
It is believed that catheterization of the internal jugular vein is accompanied by fewer complications (thrombosis, bleeding) compared to catheterization of the subclavian vein. At the same time, in some cases it is more convenient to use the subclavian approach, for example: with hypovolemia, motor agitation, low blood pressure in the patient, etc.
Femoral vein catheterization is associated with an increased risk of infectious and thrombotic complications. And it is used as a backup option if it is impossible to perform central catheterization from another access. To facilitate the search for a vein and reduce the risk of complications, ultrasound examination allows us to clarify the individual characteristics of the location of the patient’s venous trunks.
Attention!
If an attempt to catheterize a vein ends in failure, do not persist and immediately call a colleague for help - it often helps, if not to solve the problem, then at least to avoid troubles in the future.
Central venous catheterization
Catheterization of the subclavian vein
When catheterizing the subclavian vein (with “subclavian”, in the slang of anesthesiologists), the following algorithm is performed:
catheterization of the subclavian vein
Place the patient on his back with his head turned in the direction opposite to the catheterization and with his arm lying along the body on the side of the catheterization,
- Carry out local anesthesia of the skin according to the infiltration type (lidocaine, novocaine) from below the collarbone at the border between its inner and middle thirds,
- Using a long needle, into the lumen of which a conductor (introducer) is inserted, make an injection between the first rib and the collarbone and thus ensure entry into the subclavian vein - this is the basis for the Seldinger method of catheterization of central veins (insertion of a catheter using a conductor),
- Check for the presence of venous blood in the syringe,
- Remove the needle from the vein,
- Insert a catheter into the vein using a guidewire and secure the outer part of the catheter with several sutures to the skin.
Video: catheterization of the subclavian vein - training video
Catheterization of the internal jugular vein
catheterization of the internal jugular vein
Puncture of the right internal jugular vein through central access
Place the patient on his back, arms along the body, turn his head to the left. To increase the filling of the central veins and reduce the risk of air embolism, place the Trendelenburg position (the head end of the table is lowered 15° down), if the bed design does not allow this, place it horizontally.
Determine the position of the right carotid artery. The internal jugular vein is located more superficially, lateral and parallel to the carotid artery. Treat the skin with an antiseptic and limit the puncture site with sterile wipes. Infiltrate the skin and subcutaneous tissue over the anterior edge of the sternocleidomastoid muscle at the level of the thyroid cartilage with 5 ml of 1% lidocaine solution. A search puncture is performed with an intramuscular needle in order to localize the location of the vein with minimal risk of significant bleeding due to unintentional puncture of the artery.
You should also use a “search needle” if there is coagulopathy, or the puncture needle from the set is inconvenient for you, or you need to insert a large-diameter catheter. If you have good manual skills, you can naturally refuse to use the “search puncture”. With your left hand, determine the course of the carotid artery. Insert the needle slightly lateral (approximately 1 cm) of the artery at a 45° angle to the skin towards the right nipple in men or the right superior anterior iliac spine in women. Advance the needle slowly, maintaining a vacuum in the syringe, until blood is drawn. The vein is located superficially, so you should not insert the needle deeper than 3-4 centimeters.
If you do not find a vein, slowly withdraw the needle under the skin, maintaining a vacuum in the syringe (since the needle could accidentally puncture both walls of the vein). If you are unable to obtain blood, try again, this time taking a slightly more medial direction. Once you are sure that you have found a vein, you can remove the search needle, remembering the direction of the puncture, or leave it in place, removing it after the needle from the set hits the vein. Venous puncture with a needle from the set is performed in the direction determined during the search puncture.
Contraindications
Contraindications for central venous catheterization are:
- Blood clotting disorder;
- Inflammatory at the puncture site;
- Clavicle injury;
- Bilateral pneumothorax and some others.
However, you need to understand that contraindications are relative, because if a catheter needs to be inserted for health reasons, then this will be done under any circumstances, because To save a person’s life in an emergency, venous access is needed)
For catheterization of central (main) veins, one of the following methods can be selected:
1. Through the peripheral veins of the upper limb, usually the elbow. The advantage in this case is the ease of execution; the catheter is passed to the mouth of the superior vena cava. The disadvantage is that the catheter can remain in place for no more than two to three days.
We also recommend reading: Anesthesia for tattooing
2. Through the subclavian vein on the right or left.
3. Through the internal jugular vein, also on the right or left.
Complications of central venous catheterization include the occurrence of phlebitis and thrombophlebitis.
For puncture catheterization of the central veins: jugular, subclavian (and, by the way, arteries), the Seldinger method (with a guide) is used, the essence of which is as follows:
1. A vein is punctured with a needle, a conductor is passed through it to a depth of 10 - 12 cm,
2. Next, the needle is removed, a catheter is passed through the guidewire,
3. After this, the guide is removed, the catheter is fixed to the skin with a bandage.
Puncture of the right subclavian vein
Place the patient on his back, arms along the body, turn his head to the left. To move your shoulders back and down, place a bolster between your shoulder blades. To increase the filling of the central veins and reduce the risk, place the Trendelenburg position (the head end of the table is lowered 15° downwards), if the bed design does not allow this - horizontal.
Feel the jugular notch of the sternum, sternoclavicular and acromioclavicular joints. Next, treat the skin with an antiseptic solution and limit the puncture site with sterile wipes. The puncture point is located 2-3 cm below the clavicle, on the border of the middle and medial thirds of it. Infiltrate the skin and subcutaneous tissue around the puncture site with 5-10 ml of 1% lidocaine solution.
Insert the needle through the indicated point until it touches the collarbone. Gradually push the end of the needle down until it is just below your collarbone. Then rotate and point the needle at the jugular notch. Slowly advance the needle forward, maintaining a vacuum in the syringe, until blood is drawn. The bevel of the end of the needle should be turned towards the heart - this increases the likelihood of correct installation of the catheter. Try to keep the needle parallel to the plane of the bed (to avoid puncture of the subclavian artery or pleura);
If you miss a vein, slowly withdraw the needle under the skin while maintaining vacuum in the syringe. Rinse the needle and make sure it is clear. Try again, taking the injection direction a little more cranial.
Catheterization of veins and arteries
Catheterization of the subclavian vein opens up truly broad opportunities in the treatment, prevention and improvement of the quality of life of patients. Installing a permanent venous access brings less discomfort and pain to patients, and makes it easier for staff to carry out medical appointments.
Indications
A central intravenous catheter is installed if necessary:
- in monitoring central venous pressure;
- long-term administration of antibiotics;
- long-term parenteral nutrition in chronic patients;
- chemotherapy;
- administration of drugs that cause phlebitis;
- plasmapheresis and dialysis;
- blood transfusion, rehydration.
The subclavian vein is most often catheterized, since it is quite large and has convenient supraclavicular or subclavian access.
If it is still impossible to place a catheter in the subclavian vein, then catheterization of the internal and external jugular or femoral veins is performed. Possible techniques for performing the procedure are described by M.
Rosen in the author's manual "Percutaneous catheterization of central veins."
Methodology
The technique of catheterization of the subclavian vein involves positioning the patient on his back so that the head is lowered approximately 15-20 degrees relative to the body. This is necessary to prevent air embolism.
You are asked to stretch your arms along the body, and turn your head in the direction opposite to where the procedure will be performed.
Another method of giving the body the correct position is to place a roller along the spine in the area between the shoulder blades, with the arm on the catheterization side extended and pressed against the body.
Stages of installing a venous catheter according to Seldinger: a) a puncture of the vessel is made with a needle; b) a guidewire is placed through the needle into the vein, and the needle is removed; c) a catheter is threaded onto the guidewire; d) the catheter is inserted into the vessel and the guidewire is removed
The surgical field is treated extensively according to the sanitary and epidemiological regime - three times with an antiseptic solution. Next, it is covered with a sterile napkin or diaper so that the entire surface with which the doctor’s hand comes into contact is isolated. Only the injection site remains free. He is treated with an antiseptic for the fourth time.
We also recommend reading: Algorithm for taking blood from a vein
Then a solution of novocaine is drawn into the syringe and infiltrating anesthesia of the skin and subcutaneous tissue is performed. Then novocaine is added to the syringe, a needle is attached to catheterize the subclavian vein, and an injection is made between the first rib and the collarbone. The needle is directed towards the jugular notch.
Control of the needle entering the vein is carried out by pulling back the piston, and blood should appear in the syringe. The syringe is disconnected, and the needle hole is clamped with a finger to prevent embolism. A conductor is installed through the needle to a depth of 12 cm, usually a metal or plastic fishing line. After this, the needle is removed.
An expander is first inserted through the conductor, increasing the diameter of the channel between the collarbone and the rib; it does not enter the vessel.
Then the dilator is removed, and catheterization of the subclavian vein is carried out according to Seldinger - the catheter is inserted into the vein along the conductor with a screwing motion, and the conductor is removed. Check that the catheter is in the vein (blood should flow into the attached syringe).
After this, the catheter is washed with an isotonic solution to prevent complications in the form of blood clots and an infusion system is connected, or the hole is closed with a sterile cap. The free edge of the catheter is fixed to the skin by sewing with silk ligatures.
Set for catheterization of central veins according to Seldinger from bottom to top: catheter, dilator (dilator), needle, scalpel, syringe, conductor
Thus, a kit for catheterization of central veins according to Seldinger should contain: novocaine solution, heparin (5000 U/ml), antiseptics - iodine solution and alcohol 70°, 10 ml syringe, injection needles, catheterization needle, a suture needle with suture material, surgical clamps and holders, sterile napkins, diapers, dressing material, an intravenous catheter and a guidewire of the appropriate size for the lumen of the catheter.
Complications
Installation of a catheter in the central veins may be accompanied by some complications - atrial and ventricular arrhythmia; hematomas; pneumo- and hemothorax; perforation of a vein; damage to the trachea, nerve trunks, heart.
Catheter device for central venous access Certofix
Some complications can be managed with high-quality Certofix catheters. They have a soft tip (1) made of polyurethane, which prevents perforation of blood vessels and damage to the intima. Also scale (2) to determine the length of the intracorporeal section of the catheter. They are made of radiopaque material, which allows for X-ray control of its placement in the vessel.
If there are multiple channels, they are color coded (3) to identify the distal, middle and proximal channels. In addition to the fixing wings, each channel has a movable clamp (4) - a clamp, which allows you to avoid turning or dislodging the catheter.
There is also a self-closing system (5) which reduces the risk of air embolism or blood leakage.
Alternative
In world practice, there has been a tendency to move away from catheterization of the main veins. Almost all problems of intravenous therapy can be more safely solved by catheterization of a peripheral vein.
This method causes virtually no complications with proper installation and maintenance.
Catheterization of a peripheral vein allows the administration of drugs that the patient cannot take orally, and accurately dose the concentration of the drug in the bloodstream; provide frequent courses of intravenous therapy; administer medications in a stream, monitor blood pressure; provide parenteral nutrition and rehydration.
In addition, you can choose a place on the patient’s body where the device will not cause discomfort, and if necessary, its location can be changed.
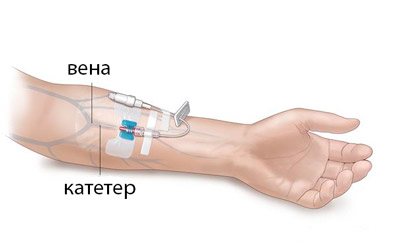
Catheterization of a peripheral vein is carried out on large vessels of straight sections of the body.
As a rule, these veins are located inside or outside the forearm (most often we are talking about the cubital vein in the cubital fossa), and if they are inaccessible, then they use the vessels of the metacarpus or dorsum of the foot, or the temporal veins in infants.
One of the main tasks is the correct selection of the diameter of the catheter for intravenous puncture. The smallest size that will accomplish the medical task should be used.
Algorithm of actions when placing a peripheral venous catheter
The location of the catheter is first determined. A tourniquet is applied above this place and when the veins are full, a vessel suitable for the procedure is selected. Treat the skin with an antiseptic, rubbing in the direction of the tourniquet. Take the guide needle and enter the skin at an angle of 15 degrees, and once it enters the vein, parallel.
The presence in the vessel is checked by the appearance of blood in the control chamber. The guide needle is pulled towards you, and the catheter is moved from the needle into the vein. Remove the tourniquet. The inlet is either closed with a sterile cap or an infusion system is attached. It is fixed on the skin by gluing the wings of the device using a special patch.
To prevent thrombosis, the catheter is flushed with an isotonic solution through the upper injection port.
Catheter for peripheral veins disassembled A. and assembled B.: 1-needle guide, 2-sterile plug, 3-cap, 4-catheter, 5-upper port
Arterial catheterization
The purpose of this procedure is different from the purpose of central venous catheterization. By providing constant access to the arterial part of the circulatory system using a catheter, it is possible to dynamically monitor the pressure and gas composition of the blood.
The most accurate readings can be taken during femoral artery catheterization, especially if severe hypotension occurs. If there is no severe hypotension, then it is quite possible to install a catheter in the radial artery. But first, a test should be carried out to assess the development of the bypass vascular bed.
If it is insufficient, then this installation site should be abandoned, since the sections located below the device will be insufficiently supplied with blood and experience hypoxia.
An arterial catheter can also be placed over a guidewire using the Seldinger technique. It is made of tissue and blood compatible material, has a smooth surface that prevents the formation of blood clots, and a locking fitting for combination with the Luer system
The catheterization protocol involves the use of a catheter on a 20 G needle. The procedure takes place under aseptic conditions. The puncture site is anesthetized, and under digital control of the pulse wave, a cannula on a yoke is inserted into the artery.
When placed correctly, a scarlet stream of blood beats from the open end in time with the pulse. The needle is removed, and the device remains in the vessel, it is washed with an isotonic solution and a pressure monitoring device is attached. So, the arterial curve is recorded.
The catheter can be sutured to the skin or secured with a bandage that limits wrist flexion and holds the system securely in place.
Catheter Care
Prevention of complications when a subclavian or peripheral venous catheter is installed goes in several directions.
- Combating vascular thrombosis. Every 4-6 hours the catheter must be flushed with saline solution with the addition of heparin.
- Prevention of infection around the entrance hole. Firstly, the procedure is carried out according to the rules of the operation, and secondly, the skin around the puncture site is treated every day with a solution of alcohol or Lugol, possibly alternating with treatment with a solution of chloramine or boric acid.
- Prevention of vascular injury from catheter displacement.
- Prevention of air embolism with negative venous pressure.
The correct technique for catheterization of veins and arteries, as well as high-quality care, allows catheters to remain in the patient’s body for a long time and safely and provide the full range of treatment measures.
Source: https://icvtormet.ru/prochee/kateterizaciya-ven-arteriy
Puncture of the right femoral vein
Position the patient on his back, with a cushion placed under the buttocks. The leg should be slightly abducted and turned outward. Determine the pulsation of the femoral artery below the inguinal ligament: the femoral vein is located more medially. Treat the skin with an antiseptic and limit the puncture site with sterile wipes. Next, infiltrate the skin and subcutaneous tissue with 5 ml of a 1% lidocaine solution. Incise the skin with a scalpel with a small blade.
2 cm below the inguinal ligament, determine the course of the femoral artery with two fingers of your left hand. The needle is inserted 1 cm medial to the femoral artery at an angle of 30° to the skin and directed along the vein, maintaining a vacuum in the syringe until blood is obtained. The vein is usually located at a depth of 2-4 cm from the surface of the skin. It is convenient to use a G14-16 peripheral venous catheter as a needle, after making sure that it passes the conductor.
If you do not find a vein, slowly remove the needle while maintaining a vacuum in the syringe. Rinse the needle and make sure it is clear. Try again, aiming the needle slightly to the right or left of the original puncture site.
Catheter placement
Catheterization of central veins and peripheral vessels is allowed only in departments of medical institutions. The procedure is performed by a vascular surgeon, anesthesiologist, or interventional radiologist. Before inserting a catheter into a vein, medical workers prepare:
- determine the presence of allergic reactions to administered drugs;
- analyze the degree and speed of blood clotting;
- drugs are prescribed to prevent thrombosis.
If it is planned to place a catheter on a woman, the doctor is obliged to determine the presence or absence of pregnancy.
The final stage of the central venous catheterization procedure is suturing and fixing the device to the skin. A locking cap is placed on the inlet of the catheter. The catheter is then covered with a sterile dressing, on which the current date is stamped. This is necessary to track the period how long you can keep the catheter without reinstallation.
Catheterization of the subclavian vein
The success rate of puncture and catheterization of the subclavian vein reaches 99-100%. The vessel has a fairly large diameter; getting into it is not difficult. Performing puncture and catheterization of the subclavian veins is standard. The patient is placed on the operating table on his back, his head tilted to the side so that the doctor has free access to the injection site.
After local anesthesia, the doctor inserts a needle under the collarbone to a depth of about 4 cm until the costoclavicular ligament is pierced. After this, the needle advance slows down. When the subclavian vein is punctured, the doctor feels another dip in the needle.
To prevent embolism from occurring during puncture and catheterization of the subclavian vein, the patient should slightly hold back his or her breaths after puncture. The syringe is removed, but the needle remains in place. A conductor is inserted into it, after which the needle is removed, and the catheter is guided onto the remaining guide line using rotational movements. After reaching the required depth, the conductor is removed. The process of puncture and catheterization of the subclavian vein is completed by washing the device tube with saline and fixing it to the skin with silk sutures.
With proper care of the catheter, it can remain in place for up to 2-3 months.
Catheterization of the internal jugular vein
When catheterizing the internal jugular vein (abbreviated as IJV), it is important to be precise and careful with the needle placement. The slightest inaccuracy will lead to rupture of the wall of the carotid artery.
The technique of catheterization of the internal jugular vein involves preliminary anesthesia of the tissues in the area of catheter insertion. As in the previous case, this is done using a 10-gram syringe with anesthetic. The drug is injected into the subcutaneous tissue in the area of the sternocleidomastoid muscles, 5-10 mm outward from the place where the collarbone connects to the sternum. At this point, the jugular vein is located as close to the surface as possible.
As the needle immerses, the doctor should feel two “failures”: when passing through the fascia of the neck and at the moment of penetration through the wall of the vessel. After the second failure, the speed of needle advancement is significantly reduced, and then the steps are repeated to install the guidewire and catheter.
Femoral vein catheterization
Catheterization of the femoral vein begins with the administration of an anesthetic. The doctor places the needle at an angle of 45 degrees to the surface of the skin outward from the place where the pulsation of the femoral artery is felt, that is, on the midline between the pubic fusion and the upper border of the ilium. The needle is inserted to a depth of 2-4 cm until it “falls through”.
Once the needle enters the femoral vessel, it is important to remove the plunger and ensure that it is in a vein and not an artery.
Peripheral vein catheterization
Anesthesiologists and vascular surgeons consider catheterization of peripheral veins to be the simplest procedure, the algorithm of which differs significantly from the insertion of tubes into the central vessels. The procedure does not require local anesthesia. To improve vessel visualization, catheterization of peripheral veins begins with applying a tourniquet above the puncture site. After the contour swells, the doctor inserts a cannula into it at a slight angle. When the needle enters the lumen of a blood tube, dark blood is visible on the needle in the imaging chamber. A catheter for peripheral veins is inserted through the needle. The outer end of the tube is fixed to the skin with an adhesive plaster.
Umbilical vein catheterization
The availability and sufficient size of the umbilical vessels in newborns allows them to be used for measuring hemodynamic parameters, administering nutrients and drugs. The technique of the procedure is somewhat different from others. Before catheterization of the umbilical vein is carried out, it is necessary to prepare the intervention area: treat the field with antiseptics, free the mouth in the umbilical cord stump from blood clots. A catheter is inserted into the lumen of the vein, while simultaneously aspirating the vessel to remove blood clots. With a uniform blood flow, the tube is inserted to the required depth, fixed in the stump and a sterile bandage is applied.
Seldinger catheter insertion
Immediately after puncture of the vein, make sure that the blood flows easily into the syringe. Disconnect the syringe while holding the needle in place. Try to rest your hand on the patient’s body to minimize the risk of needle migration from the lumen of the vein. Close the needle pavilion with your finger to prevent air from entering;
Insert the flexible end of the guidewire into the needle. If there is any resistance to the conductor's advance, carefully turn it and try to advance it. If this does not help, remove the metal conductor. Assess blood aspiration from the vein again. Change the angle of the needle or rotate it, check the flow of blood into the syringe. Try again. If it was not possible to insert a plastic conductor, in order to avoid cutting, it must be removed along with the needle.
After inserting the guidewire halfway into the vein, remove the needle. Before inserting the dilator, incise the skin with a scalpel with a small blade; Insert a dilator through the guidewire. Try to take the dilator with your fingers closer to the skin to avoid bending the conductor and additional trauma to the tissue, or even the vein. There is no need to insert the dilator over its entire length; it is enough to create a tunnel in the skin and subcutaneous tissue without penetrating the lumen of the vein. Remove the dilator and insert the catheter. Remove the conductor. Perform an aspiration test. Free blood flow indicates that the catheter is in the lumen of the vein.
Peripheral vein catheterization
Of the peripheral veins, the most preferable in terms of puncture are the lateral and medial vein of the forearm, the intermediate ulnar vein, and the vein on the back of the hand.
peripheral vein catheterization
The algorithm for inserting a catheter into a vein in the arm is as follows:
- After treating the hands with antiseptic solutions, the required catheter size is selected. Typically, catheters are marked according to size and have different colors - purple for the shortest catheters with a small diameter, and orange for the longest with a large diameter.
- A tourniquet is applied to the patient's shoulder above the catheterization site.
- The patient is asked to “work” with his fist, squeezing and unclenching his fingers.
- After palpation of the vein, the skin is treated with an antiseptic.
- A puncture of the skin and vein is performed with a stiletto needle.
- The stiletto needle is pulled out of the vein while the catheter cannula is inserted into the vein.
- Next, a system for intravenous infusions is connected to the catheter and medicinal solutions are infused.
Video: puncture and catheterization of the ulnar vein
Monitoring the correct position of the distal end of the jugular or subclavian catheter
The end of the catheter should be in the vena cava. If the catheter is located high in the upper part of the vena cava, its end may rest against the opposite wall of the vein, which complicates infusions and contributes to the formation of a parietal thrombus. The presence of a catheter in the cavities of the heart causes rhythm disturbances and increases the risk of cardiac perforation.
Installation of a catheter under ECG control allows you to optimize its position and reduce the likelihood of complications.
1. The catheter is washed with saline solution. A metal conductor is inserted into the catheter so that it does not extend beyond the catheter (some conductors have a special mark). Or a metal intramuscular needle is inserted through the catheter plug and the catheter is filled with a 7.5% solution. A plug is put on the needle;
2. Attach the chest lead “V” wire of the electrocardiograph or cardioscope to the needle or conductor using an alligator clip. And turn on the “thoracic abduction” mode on the recording device. Or connect the wire of the right hand to the distal electrode and turn on the second (II) lead on the cardioscope or cardiograph;
3. If the end of the catheter is in the right ventricle, we see a high-amplitude (5-10 times larger than usual) QRS complex on the monitor screen. Slowly tightening the catheter, we see a decrease in the amplitude of the QRS complex, but the P wave remains very high, which indicates that the catheter is in the atrium.
Further tightening of the catheter leads to normalization of the amplitude of the P wave. We tighten the catheter approximately 1 cm more - this is the optimal position of the catheter in the superior vena cava.
4. Secure the catheter to the skin with a suture or adhesive tape. Apply a sterile dressing.
Seldinger technique for catheterization of the subclavian vein
INDICATIONS for catheterization may include:
• inaccessibility of peripheral veins for infusion therapy;
• long operations with large blood loss;
• the need for large volumes of infusion therapy;
• the need for parenteral nutrition, including the transfusion of concentrated, hypertonic solutions;
• the need for diagnostic and control studies to measure CVP (central venous pressure).
CONTRAINDICATIONS to PV catheterization are:
• superior vena cava syndrome:
• Paget-Schroeter syndrome (acute subclavian vein thrombosis);
• sudden disturbances of the blood coagulation system towards hypocoagulation;
• local inflammatory processes at the sites of venous catheterization;
• severe respiratory failure with pulmonary emphysema;
• bilateral pneumothorax;
• trauma to the clavicle area.
In case of unsuccessful CPV or its impossibility, internal and external jugular or femoral veins are used for catheterization.
The subclavian vein starts from the lower border of the 1st rib, goes around it from above, deviates inwards, downwards and slightly forward at the place of attachment to the 1st rib of the anterior scalene muscle and enters the chest cavity.
Behind the sternoclavicular joint they connect with the internal jugular vein and form the brachiocephalic vein, which in the mediastinum with the same left side forms the superior vena cava. In front of the PV is the collarbone.
The highest point of the PV is anatomically determined at the level of the middle of the clavicle at its upper border.
Laterally from the middle of the clavicle, the vein is located anterior and inferior to the subclavian artery. Medially behind the vein there are bundles of the anterior scalene muscle, the subclavian artery and, then, the dome of the pleura, which rises above the sternal end of the clavicle. The PV passes anterior to the phrenic nerve. On the left, the thoracic lymphatic duct flows into the brachiocephalic vein.
For CPV, the following drugs are required: • novocaine solution 0.25% - 100 ml; • heparin solution (5000 units in 1 ml) – 5 ml; • 2% iodine solution; • 70° alcohol; • antiseptic for treating the hands of a doctor performing an operation; • cleol.
sterile instruments: • pointed scalpel; • syringe 10 ml; • injection needles (subcutaneous, intravenous) – 4 pieces; • needle for puncture catheterization of veins; • surgical needle; • needle holder; • scissors; • surgical clamps and tweezers, 2 pieces each; • intravenous catheter with a cannula, plug and conductor, respectively, the thickness of the diameter of the internal lumen of the catheter and twice its length; • container for anesthetic, • bag with a sheet, diaper, gauze mask, surgical gloves, dressings (balls, napkins).
Catheterization technique
The room where CPV is performed must be in a sterile operating room: dressing room, intensive care unit or operating room.
In preparation for CPV, the patient is placed on the operating table with the head lowered by 15° to prevent air embolism.
The head is turned in the direction opposite to the one being punctured, the arms are extended along the body. Under sterile conditions, a hundred is covered with the above instruments. The doctor washes his hands as before a normal operation and puts on gloves. The surgical field is treated twice with a 2% iodine solution, covered with a sterile diaper and treated again with 70° alcohol.
Subclavian access •• A 0.5% procaine solution is injected intradermally with a syringe with a thin needle to create a “lemon peel” at a point located 1 cm below the clavicle on the line separating the middle and inner third of the clavicle. The needle is advanced medially towards the upper edge of the sternoclavicular joint, continuously applying procaine solution.
The needle is passed under the collarbone and the rest of the procaine is injected there. The needle is removed •• Using a thick sharp needle, limiting the depth of its insertion with the index finger, the skin is pierced to a depth of 1–1.5 cm at the location of the “lemon peel”.
The needle is removed •• A syringe with a capacity of 20 ml is filled up to half with 0.9% sodium chloride solution, and a not very sharp (to avoid puncture of the artery) needle 7–10 cm long with a bluntly beveled end is put on. The direction of the bevel should be marked on the cannula. When inserting the needle, its bevel should be oriented in the caudal-medial direction.
The needle is inserted into a puncture previously made with a sharp needle (see above), and the depth of possible needle insertion should be limited to the index finger (no more than 2 cm). The needle is advanced medially towards the upper edge of the sternoclavicular joint, periodically pulling the plunger back, checking the flow of blood into the syringe.
If unsuccessful, the needle is pushed back without removing it completely, and the attempt is repeated, changing the direction of advancement by several degrees. As soon as blood appears in the syringe, part of it is injected back into the vein and again sucked into the syringe, trying to obtain a reliable reverse blood flow.
If a positive result is obtained, ask the patient to hold his breath and remove the syringe from the needle, squeezing its hole with a finger. •• A conductor is inserted into the needle with light screwing movements halfway; its length is slightly more than two times the length of the catheter.
The patient is again asked to hold his breath, the guide is removed, closing the catheter hole with a finger, then a rubber stopper is put on the latter. After this, the patient is allowed to breathe. If the patient is unconscious, all manipulations associated with depressurization of the lumen of the needle or catheter located in the subclavian vein are performed during exhalation •• The catheter is connected to the infusion system and fixed to the skin with a single silk suture. Apply an aseptic dressing.
Complications with CPV
Incorrect position of the guidewire and catheter.
It leads to:
– heart rhythm disturbances;
– perforation of the wall of the vein, heart;
– migration through the veins;
– paravasal administration of fluid (hydrothorax, infusion into the fiber);
– twisting of the catheter and formation of a knot on it.
In these cases, correction of the position of the catheter, assistance from consultants, and possibly removal of it are required to avoid worsening the patient's condition.
Puncture of the subclavian artery usually does not lead to serious consequences if it is promptly identified by pulsating bright red blood.
To avoid air embolism, it is necessary to maintain the tightness of the system. After catheterization, a chest X-ray is usually ordered to rule out possible pneumothorax.
If the catheter is left in the PV for a long time, the following complications may occur:
• vein thrombosis.
• catheter thrombosis,
• thrombo- and air embolism, infectious complications (5 – 40%), such as suppuration, sepsis, etc.
To prevent these complications, it is necessary to properly care for the catheter. Before all manipulations, you should wash your hands with soap, dry them and treat them with 70° alcohol. To prevent AIDS and serum hepatitis, wear sterile rubber gloves.
The sticker is changed daily, and the skin around the catheter is treated with 2% iodine solution, 1% brilliant green solution, or methylene blue. The infusion system is changed daily. The catheter is flushed with a heparin solution after each use to create a “heparin lock”. It is necessary to ensure that the catheter is not filled with blood.
The catheter is changed using a guide every 5–10 days to prevent complications. If such occurs, the catheter is removed immediately.
Thus, CPV is a rather complex operation, which has its own indications and contraindications.
Due to the individual characteristics of the patient, violation of catheterization technique, omissions in caring for the catheter, complications may arise with harm to the patient, therefore, instructions have been created for all levels of medical personnel related to this (attending physician, team performing CPV, nurse in the manipulation room). All complications must be recorded and discussed in detail in the department.
Access to the PV can be either subclavian or supraclavicular. The first is the most common (probably due to its earlier implementation). There are many points for puncture and catheterization of the subclavian vein, some of them (named by authors) are shown in the figure
The Abaniak point is widely used, which is located 1 cm below the collarbone along the line dividing the inner and middle third of the clavicle (in the subclavian fossa).
From my own experience, the point can be found (this is especially important in obese patients) if the second finger of the left hand (with CPV on the left) is placed in the suvarar notch of the sternum, and the first and third fingers slide along the lower and upper edges of the clavicle until the first finger hits the subclavian fossa.
The needle for puncture of the PV should be directed at an angle of 45 to the clavicle into the projection of the sternoclavicular joint between the clavicle and the 1st rib (along the line connecting the first and second fingers); it should not be punctured deeper.
RECOGNITION OF ARTERY PUNCTURE AND PREVENTION OF AIR EMBOLISM.
In all patients with normal blood pressure and normal oxygen tension in the blood, arterial puncture is easily recognized by the pulsating stream and bright red color of the blood.
However, in patients with profound hypotension or significant arterial desaturation, these signs may be absent.
If there is any doubt about where the guide needle is located - in a vein or artery, a single-lumen number 18 catheter, available in most kits, should be inserted into the vessel over a metal guide. This step does not require the use of an extender.
The catheter can be connected to a pressure transducer to identify the venous pulse wave and venous pressure. It is possible to take two identical blood samples at the same time to determine blood gases from the catheter and from any other artery. If the gas content is significantly different, the catheter is in the vein.
Patients with spontaneous breathing have negative venous pressure in the chest at the moment of inspiration. If the catheter is in free communication with outside air, this negative pressure can draw air into the vein, resulting in an air embolism.
Even a small amount of air can be fatal, especially if it is transferred into the systemic circulation through an atrial or ventricular septal defect.
To prevent such a complication, the mouth of the catheter must be closed at all times, and at the time of catheterization the patient must be in the Trandelenburg position.
If an air embolism does occur, in order to prevent air from entering the outflow tract of the right ventricle, the patient should be placed in the Trandelenburg position with the body tilted to the left. To speed up air resorption, 100% oxygen should be prescribed. If the catheter is in the heart cavity, air aspiration should be used.
PREVENTIONAL PRESCRIPTION OF ANTIBIOTICS.
Most studies of prophylactic antibiotic use have shown that this strategy was associated with a reduction in infectious complications involving the bloodstream. However, the use of antibiotics is not recommended, since it promotes the activation of microorganisms sensitive to antibiotics.
Care of the manipulation site
OINTMENTS, SUBCUTANEOUS CUFFS AND BANDAGES
Applying an antibiotic ointment (eg, basithramycin, mupirocin, neomycin, or polymyxin) to the catheter site increases the incidence of fungal colonization of the catheter, promotes the activation of antibiotic-resistant bacteria, and does not reduce the number of catheter-related infections involving the bloodstream. These ointments should not be used.
Likewise, the use of silver-impregnated subcutaneous cuffs does not reduce the incidence of catheter-related bloodstream infections and is therefore not recommended.
Because evidence is conflicting regarding the optimal type of dressing (gauze versus clear materials) and the optimal frequency of dressing changes, evidence-based recommendations cannot be formulated.
Source: https://zhardem.kz/news/3760
Complications
Arterial puncture
If you accidentally puncture an artery, apply pressure to the puncture site for 5-10 minutes, then repeat venipuncture.
Pneumothorax/hydrothorax
A patient on mechanical ventilation may develop tension pneumothorax. In this case, even with a small pneumothorax, drainage of the pleural cavity is necessary. If the patient is breathing on his own, with a small pneumothorax, dynamic observation is carried out. If there are large signs of respiratory failure, drain the pleural cavity.
Hydrothorax is most often associated with the end of the catheter being in the pleural cavity. Sometimes the fluid can be evacuated through this incorrectly installed catheter by lowering the head end of the table or bed.
Displacement of the subclavian catheter into the internal jugular vein
The position of the catheter should be changed, since the introduction of hypertonic solutions into the internal jugular vein can cause venous thrombosis.
Frequent ventricular extrasystoles or ventricular tachycardia
The development of these arrhythmias may indicate that the tip of the catheter is directly on the tricuspid valve. Pull the catheter back a few centimeters.
Catheter infection
The most common infection is Staphylococcus aureus
and
S. epidermidis,
but in patients with immunodeficiency, the causative agents of infection can be gram-negative rods or fungi.
Clear signs of infection
catheter: soreness, redness of the skin and purulent discharge at the site of the catheter.
Possible catheter infection
: in the presence of fever or other systemic signs, but no signs of infection at the catheter site.
In all cases, the catheter must be removed
, and send its end for bacteriological culture and prescribe antibiotics.
The easiest and fastest way to gain access to administer medications is to perform catheterization. Large and central vessels such as the internal superior vena cava or the jugular vein are mainly used. If there is no access to them, then alternative options are found.
Why is it carried out?
The femoral vein is located in the groin area and is one of the large highways that carries out the outflow of blood from the lower extremities of a person.
Catheterization of the femoral vein saves lives, since it is located in an accessible place, and in 95% of cases the manipulations are successful.
Indications for this procedure are:
- impossibility of administering drugs into the jugular or superior vena cava;
- hemodialysis;
- carrying out resuscitation actions;
- vascular diagnostics (angiography);
- the need for infusions;
- cardiac stimulation;
- low blood pressure with unstable hemodynamics.
Indications and contraindications
The following indications for central venous catheterization are distinguished:
- Complex operations with possible massive blood loss;
- Open heart surgery with AIC and in general on the heart;
- The need for intensive care;
- Parenteral nutrition;
- Possibility of measuring CVP (central venous pressure);
- Possibility of taking multiple blood samples for control;
- Introduction of a cardiac pacemaker;
- X-ray and contrast examination of the heart;
- Probing of the cavities of the heart.
Preparation for the procedure
For femoral vein puncture, the patient is placed on the couch in a supine position and asked to stretch his legs and slightly spread them. Place a rubber cushion or pillow under your lower back. The skin surface is treated with an aseptic solution, hair is shaved off if necessary, and the injection site is limited with sterile material. Before using the needle, locate the vein with your finger and check for pulsation.
The procedure includes:
- sterile gloves, bandages, napkins;
- pain reliever;
- 25 gauge catheterization needles, syringes;
- needle size 18;
- catheter, flexible guidewire, dilator;
- scalpel, suture material.
Items for catheterization must be sterile and within the reach of the doctor or nurse.
Technique, Seldinger catheter insertion
Seldinger is a Swedish radiologist who in 1953 developed a method for catheterizing large vessels using a guidewire and a needle.
Puncture of the femoral artery using his method is still carried out today:
- The space between the symphysis pubis and the anterior iliac spine is conventionally divided into three parts. The femoral artery is located at the junction of the medial and middle third of this area. The vessel should be moved laterally, since the vein runs parallel.
- The puncture site is punctured on both sides, giving subcutaneous anesthesia with lidocaine or another anesthetic.
- The needle is inserted at an angle of 45 degrees at the site of vein pulsation, in the area of the inguinal ligament.
- When dark cherry-colored blood appears, the puncture needle is moved along the vessel 2 mm. If blood does not appear, you must repeat the procedure from the beginning.
- The needle is held motionless with the left hand. A flexible conductor is inserted into its cannula and advanced through the cut into the vein. Nothing should interfere with the movement into the vessel; if there is resistance, it is necessary to slightly turn the instrument.
- After successful insertion, the needle is removed, pressing the injection site to avoid hematoma.
- A dilator is put on the conductor, after first excising the insertion point with a scalpel, and it is inserted into the vessel.
- The dilator is removed and the catheter is inserted to a depth of 5 cm.
- After successfully replacing the guidewire with a catheter, attach a syringe to it and pull the plunger towards you. If blood flows in, an infusion with an isotonic solution is connected and fixed. Free passage of the drug indicates that the procedure was completed correctly.
- After the manipulation, the patient is prescribed bed rest.
Angiography according to Seldinger - a method for diagnosing the condition of blood vessels
Angiography refers to an X-ray contrast study of blood vessels. This technique is used in computed tomography, fluoroscopy and radiography, the main purpose is to assess the circumferential blood flow, the condition of the vessels, as well as the extent of the pathological process.
It is important! Angiography (aortography) is used to diagnose diseases of vascular origin, developmental anomalies, tumors, parasites and other diseases.
This study should be carried out only in special X-ray angiography rooms at specialized medical institutions that have modern angiographic equipment, as well as appropriate computer equipment that can record and process the resulting images.
Hagiography is one of the most accurate medical studies.
This diagnostic method can be used in the diagnosis of coronary heart disease, renal failure, and to detect various types of cerebral circulatory disorders.
Types of aortography
In order to contrast the aorta and its branches in the case of persistent pulsation of the femoral artery, the method of percutaneous catheterization of the aorta (Seldinger angiography) is most often used; for the purpose of visual differentiation of the abdominal aorta, translumbar puncture of the aorta is used.
It is important! The technique involves the introduction of an iodine-containing water-soluble contrast agent by direct puncture of the vessel, most often through a catheter that is inserted into the femoral artery.
Seldinger catheterization technique
Percutaneous catheterization of the femoral artery according to Seldinger is performed using a special set of instruments, which includes:
- puncture needle;
- dilator;
- introducer;
- a metal conductor with a soft end;
- catheter (French size 4−5 F).
A needle is used to puncture the femoral artery to pass a metal wire in the form of a string. Then the needle is removed, and a special catheter is inserted through the guidewire into the lumen of the artery; this is called aortography.
Due to the painfulness of the manipulation, the conscious patient needs infiltration anesthesia using a solution of lidocaine and novocaine.
It is important! Percutaneous catheterization of the aorta according to Seldinger can also be performed through the axillary and brachial arteries. Passing a catheter through these arteries is often performed in cases where there is obstruction of the femoral arteries.
Seldinger angiography is considered universal in many ways, which is why it is used most often.
Installation of a catheter under ECG control
The use of this method reduces the number of post-manipulation complications and facilitates monitoring of the condition of the procedure.
, the sequence of which is as follows:
- The catheter is cleaned with an isotonic solution using a flexible guide. The needle is inserted through the plug and the tube is filled with NaCl solution.
- Lead “V” is attached to the needle cannula or secured with a clamp. The device switches on the “thoracic abduction” mode. Another method suggests connecting the wire of the right hand to the electrode and turning on lead number 2 on the cardiograph.
- When the end of the catheter is located in the right ventricle of the heart, the QRS complex on the monitor becomes higher than normal. The complex is reduced by adjusting and pulling the catheter. A tall P wave indicates the location of the device in the atrium. Further direction to a length of 1 cm leads to the alignment of the prong according to the norm and the correct location of the catheter in the vena cava.
- After the manipulations are completed, the tube is sutured or secured with a bandage.