Vasorenal hypertension (Also vasorenal arterial hypertension, renovascular hypertension) is a fairly common syndrome of high blood pressure among all age groups of both sexes, caused in most cases by disturbances of normal blood flow in the renal arteries (renal ischemia).
The processes of arterial stenosis due to atherosclerosis or fibromuscular dysplasia, arteriovenous fistulas, nonspecific aortoarteritis, thromboembolism and other diseases, complicating the normal flow of blood through the renal arteries, prevent the enzyme renin, secreted by the kidneys, from entering the arteries. This enzyme is responsible for regulating blood pressure; a decrease in its amount in the blood leads to hypertension.
Caused by hereditary or acquired arterial diseases, renovascular hypertension is usually very resistant to the effects of drugs and is usually permanent. Based on this collective characteristic, it can be distinguished from other types of arterial hypertension (high blood pressure).
1
Ultrasound in MedicCity
2 Consultation with a phlebologist in MedicCity
3 Vascular surgery in MedicCity
Regular examination by a phlebologist or vascular surgeon will help you avoid serious complications if vascular pathology is detected. Delay in treating vascular diseases is life-threatening! Trust your health to the MedicCity professionals!
Reasons for development
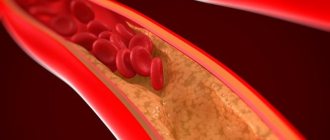
There are about forty known causes that can trigger the development of the disease. However, it is noted that the most common is atherosclerosis. Defeat against this background occurs in most people over forty years of age. Often, plaques of a malignant nature appear at the mouth of the artery. Such a lesion appears unilaterally and is capable of complications in the form of thrombosis.
A congenital disease such as fibromuscular dysplasia can also cause renovascular hypertension. The defect is a weakening of the elasticity of the walls of blood vessels, and muscle fibers turn into scar tissue. As a result, a narrowing of the lumen and a significant thickening of the walls occurs.
In addition, pathology can be provoked against the background of dystrophy or sclerotic changes. Microaneurysms can often be observed. Externally, the changes that occur can be compared to a string of beads, where narrowing and expanding sections alternately replace each other.
Among autoimmune inflammations, nonspecific aortoarteritis is identified as the cause of the development of pathology. This reason is third on the list of main ones, and the figure is equal to 10 percent of the total number of diseases. This condition is characterized by damage to the medial shell of a primary nature.
Additional reasons causing the development of pathology include:
- aneurysm;
- cysts and tumors;
- hypoplasia of the renal arteries, their abnormal development;
- thrombosis and embolism;
- extravasal compression.
In addition to those listed, there may be other reasons that provoke the manifestation of the disease.
Etiology.
There are about 40 known causes of arterial hypertension, which are divided into congenital and acquired. Among congenital ones the most common are:
• fibromuscular dysplasia of the renal arteries;
• hypoplasia of the renal artery and kidney; • extravasal compression of the renal artery; • aneurysms of the renal arteries; • arteriovenous fistulas. Acquired factors for the development of ARH:
• atherosclerosis;
• nonspecific aortoarteritis; • nephroptosis; • kidney infarction; • trauma; • dissecting aortic aneurysm. Atherosclerosis
is the main cause of renovascular hypertension in people over 40 years of age, accounting for 60-85% of cases.
Atherosclerotic plaques are localized mainly at the mouth or in the proximal third of the renal artery. In the vast majority of cases, unilateral lesions are observed, while bilateral lesions occur in approximately 1/3 of cases and lead to a more severe course of ARH. The right and left renal arteries are affected equally often. In 10% of cases, atherosclerosis of the renal arteries can be complicated by thrombosis. The disease is more common (2-3 times) in men. Fibromuscular dysplasia (FMD)
as a cause of renovascular hypertension ranks second after atherosclerosis.
It occurs mainly in young and even children (from 12 to 44 years), the average age is 28-29 years. FMD is found 4-5 times more often in women than in men. Morphologically, this pathological condition manifests itself in the form of dystrophic and sclerosing changes, affecting mainly the inner and middle lining of the renal arteries and their branches. In this case, hyperplasia of the muscular elements of the wall can be combined with the formation of microaneurysms. As a result, there is an alternation of areas of narrowing and expansion (aneurysms), which gives the arteries a unique shape - in the form of strings of pearls or beads. The pathological process, although widespread, is unilateral in 2/3 of cases. Nonspecific aortoarteritis
is in third place in frequency among the causes of ARH (up to 10%). It is characterized by a primary lesion of the medial tunic of the vessel. Inflammatory infiltration of the media with transition to the adventitia and intima ends with sclerosis and destruction of the elastic frame of the renal artery, which leads to stenosis of its lumen. The pathological process is mainly limited to the proximal segment of the vessel and almost never spreads to its intraorgan branches. In contrast to fibromuscular dysplasia, nonspecific aortoarteritis always has varying degrees of severity of aortic damage. Vasorenal hypertension can develop as a result of extravasal compression of the renal artery, as a result of thrombosis or embolism of the renal artery, aneurysm formation, hypoplasia of the main renal arteries, nephroptosis, tumors, cysts, anomalies of the kidneys, etc.
Main symptoms
As such, symptoms have not yet been identified. Complaints received from patients can only be divided into several categories:
- Characteristic signs of cerebral hypertension. This may include:
- headaches;
- heaviness felt in the back of the head;
- memory impairment;
- sleep disorders.
- Signs resulting from increased stress on the heart:
- cardiopalmus;
- heaviness in the chest.
- Symptoms of kidney damage. These include: pulling sensations in the lower back, the presence of blood and protein in the urine, dull pain.
- If other organs are affected by ischemia: lameness, weakness, carotid insufficiency.
All of the above signs indicate that this is a systemic disease.
It should also be noted that in about 25 percent of patients, the pathology passes without showing any symptoms.
Symptoms of the disease
Please note that 25% of patients with renovascular hypertension are asymptomatic. Due to the nonspecificity of symptoms, doctors face a number of difficulties when making a diagnosis. The main symptoms of renovascular hypertension:
- pain in the eyeballs;
- heaviness in the head;
- headache;
- noise in ears;
- muscle weakness;
- memory impairment;
- heartbeat disturbance;
- pain in the heart area;
- pain and heaviness in the lumbar region;
- heaviness in the chest.
Main feature
The main and often the only symptom of the disease is arterial hypertension syndrome. Its course may be no different from essential hypertension. Renal hypertension causes a persistent increase in systolic and especially diastolic blood pressure. The difference between the two indicators will always be small.
An increase in blood pressure in childhood, adolescence and young adulthood – up to 30 years – should alert you. There is a high risk of developing fibromuscular dysplasia. Patients over 45 years of age are characterized by atherosclerotic damage to the renal arteries. You should pay attention to the following symptoms of arterial hypertension:
- resistance to prescribed treatment;
- increased diastolic pressure;
- rapid damage to internal organs.
General symptoms
Signs of renovascular hypertension may vary depending on the stage, but there are a few common symptoms that most patients complain of. Such manifestations include:
- tinnitus;
- heart rhythm disturbances;
- flashing “flies” before the eyes;
- asthenic syndrome in the form of constant fatigue, depression and weakness;
- increased thirst;
- sleep disorders, insomnia;
- tightness in the chest.
Article on the topic: Treatment of cystitis in pregnant women - symptoms, diagnosis, medications and folk remedies
Diagnosis of the disease
If there is a suspicion of renovascular hypertension, it is necessary to do excretory urography. In this case, special attention should be paid to such signs as:
- Reduced contrast enhancement of the affected kidney.
- Reduced size.
- Contrasting in later periods has high rates.
If the listed symptoms occur, aortography is performed. With the help of such a study, the affected areas and their sizes are determined.
The defining method in the diagnosis of renovascular hypertension is kidney hagiography, which is carried out in special centers in this area. This method allows us to identify stenosis, its degree and location. It is these data that are the decisive factors when the question of surgical treatment arises.
Among other things, the doctor determines the pressure of the upper and lower extremities. The measurement should be carried out not only in the vertical position of the patient, but also in the horizontal position.
Diagnosis based on ultrasound involves examining the main renal arteries and analyzing the speed of blood flow through them.
Treatment methods
If the disease continues for a long time, and there is no treatment, then in 70 percent of cases the death of patients occurs within the first five years from the onset of the pathology. This is explained by the development of complications, in particular:
- stroke;
- heart attack;
- renal failure.
The use of conservative therapy in most cases does not give a positive result, and if there is an effect, it is inconsistent and lasts a short time. Even if it is possible to lower the blood pressure level, the stenosis remains. This leads to an even greater deterioration in the blood supply to the kidney. As a result, the organ shrinks a second time and completely loses its functions.
Treatment based on medication is possible only if surgery is contraindicated or in addition if the result of the operation does not lead to a decrease in pressure.
Rational therapy for renovascular hypertension is x-ray endovascular dilatation (RED) and surgical treatment.
If RED cannot be performed, surgery is performed. There are three open types:
- reconstructive method;
- conditional-reconstructive;
- nephrectomy.
As a rule, treatment of pathology resulting from nonspecific aortoarteritis is quite difficult. In this case, corrective surgery is performed not only on the artery, but also on the aorta itself.
Nephrectomy is used in cases of old thrombosis, damage to intrarenal branches and if the kidney is wrinkled. In addition, endarterectomy can be used - an operation that removes the atherosclerotic plaque that narrows the lumen of the artery.
Important! Bypass surgery is used to create an additional blood path around the vessel.
Forecast
After intravascular interventions, surgeons note a positive hypotensive effect within 6 months - in 80% of patients, 5 years - in 65%. Some patients require repeated operations.
The use of angioplasty made it possible to relieve hypertension in the first 6 months - 90% of patients, after 5 years - 73%. With existing chronic renal failure, 98% of patients survived in the first 5 years.
Undoubtedly, these indicators speak in favor of the use of surgery for the treatment of renal hypertension of vascular origin. Patients should entrust diagnostics to specialized vascular centers and not waste time and money on unnecessary tests and examinations.
Rehabilitation period
Whatever surgery is performed, it is important to remember that treatment must be continued and aimed at eliminating the underlying cause of the development of renovascular hypertension. Following some recommendations will help prevent the development of the disease:
- To give up smoking. Moreover, you should also try to avoid passive ones.
- Constant use of antiplatelet drugs (aspirin). They help thin the blood and reduce the risk of blood clots in the vessels.
- Treatment of arterial hypertension.
- Dieting to lose excess weight. Losing even four kilograms can significantly reduce blood pressure, cholesterol and blood sugar levels.
In addition, there is no need to be afraid of physical activity. You need to walk for at least one hour every day.
Renal hypertension is undoubtedly treatable. The main thing is to notice the signs of pathology in time, correctly determine the extent of its progress and undergo a course of treatment.
Vasorenal hypertension develops due to
Vasorenal hypertension
is a disease caused by narrowing of the renal arteries. The causes of their damage may be atherosclerosis (most often), fibromuscular dysplasia and nonspecific arteritis. Clinically, renovascular hypertension is manifested by stable and very high arterial hypertension. Vasorenal hypertension is relatively common, especially with fibromuscular dysplasia and arteritis, observed in young people. A characteristic feature of this type of hypertension is extreme resistance. Often hypertension takes a malignant course.
now be considered proven
that the main factor in the occurrence of hypertension during narrowing of the renal arteries is a decrease in pulsation and perfusion pressure. Under these conditions, increased secretion of renin occurs, which is formed in the juxtaglomerular apparatus of the kidneys. Then the renin-angiotensin-aldosterone system is turned on, which plays a decisive role in the development of the disease. In addition, a decrease in the production of depressor and vasodilator substances (prostaglandins, quinines, etc.) by the kidney is of known importance in the occurrence of hypertension.
Diagnosis of vasorenal hypertension
is based on a thorough general clinical examination of the patient using a number of instrumental techniques. The clinical picture consists of a triad of symptoms: hypertensive, progressive overload of the left ventricle of the heart and impaired renal function. It should be noted that the clinical picture does not have features characteristic only of renovascular hypertension. To establish a preliminary diagnosis, the following anamnestic data and clinical symptoms are of particular importance: ineffectiveness of conservative therapy or only a short-term and insignificant effect with high blood pressure numbers, young or middle age of patients with persistent high arterial hypertension, malignant course of hypertension, persistent and persistent character hypertension in persons over 40 years of age with signs of atherosclerosis in other vascular systems, systolic murmur in the projection of the renal arteries. As a rule, there are no pronounced changes in urine; The functional capacity of the kidneys is preserved.
At the next stage of diagnosis
it is necessary to exclude other types of symptomatic hypertension observed with coarctation of the aorta, pheochromocytoma, aldosteroma (Conn syndrome), etc. After excluding these diseases, they move on to more complex studies aimed at determining renal function, localization, prevalence and form of vascular damage. For this purpose, radioisotope rheography and excretory urography are performed, and finally a radiopaque study of the renal arteries - angiography. Other methods (scanning, kidney biopsy, determination of renin in peripheral blood and renal veins, thermography of the lumbar regions, etc.) are used only in cases that are especially difficult to diagnose.
Abdominal aortography
allows you to establish the nature, localization and extent of the pathological process in the renal arteries and is the main diagnostic method for renovascular hypertension. Currently, there is a tendency to expand the indications for aortography in patients with suspected occlusive lesions of the renal arteries. The most widely used method for suspected vasorsial hypertension is transfemoral aortoangiography using the Seldinger method.
Atherosclerotic stenosis
The renal artery is characterized by predominant damage to the mouth of the vessel over 1-1.5 cm with a marginal filling defect and a sharp transition from the stenotic to the unchanged portion of the vessel. Aortoarternitis is characterized by a combination of damage to the aorta and the proximal segment of the artery. The stenosis is usually circular in nature, and over a considerable extent. Post-snotic expansion is smaller than in atherosclerosis.
The only effective treatment
renovascular hypertension is early surgical intervention.
Contraindications to reconstructive operations for occlusive lesions of the renal arteries are relatively recent (up to six months) disturbances of cerebral or coronary circulation, severe decompensation of the cardiovascular system and severe renal failure, as well as extensive bilateral damage to the renal vessels, in which reconstructive surgery is technically impossible execute. The choice of surgical intervention
is made taking into account the localization, prevalence and etiology of occlusive lesions of the renal arteries.
At the All-Union Scientific Center
Surgery has developed a transortic edarterectomy from the renal artery using the eversion method. The fundamental difference between this method of operation and others is that all manipulations are performed without violating the integrity of the vascular wall of the renal artery itself. This operation is the method of choice for atherosclerosis. If the renal arteries are affected by fibromuscular dysplasia or arteritis in their proximal third, the operation of choice is resection of the vessel segment with its replantation into the aorta in an end-to-side manner; if the lesion is localized in the middle or distal third of the renal artery, resection of the vessel with end-to-end anastomosis is performed. In case of widespread damage to the renal artery, autovenous or autoarterial replacement is performed. In case of widespread damage to the artery of one kidney, when all branches are involved in the pathological process, as well as in case of atrophy or a sharp decrease in the function of one of the kidneys, a nephrectomy is performed. Short-term and long-term results indicate normalization of blood pressure in 70-85% of patients, which suggests the effectiveness of surgical treatment of renovascular hypertension.
Vasorenal hypertension develops due to
Vasorenal hypertension (RH) is a secondary (symptomatic) arterial hypertension that develops as a result of disruption of the main blood flow in the kidneys without primary damage to their parenchyma and urinary tract.
Etiology and pathogenesis. The causes of impaired blood supply to the kidneys in the vast majority of cases are: atherosclerotic process (75–80%), fibromuscular dysplasia - FMD (15%), nonspecific aortoarteritis (8–10%). These factors lead to the development of hemodynamically significant stenosis of the renal arteries and hypoperfusion of the renal glomeruli, which contributes to the activation of the renin-angiotensin-aldosterone system. In addition to a significant aggravation of systemic arterial hypertension (AH), long-term progressive hypoxia (a consequence of constant vasoconstriction) has a fibrogenic effect on kidney tissue. Fibrosis of renal tissue is accompanied by a decrease in the mass of functioning nephrons, leading to renal failure. Destruction of the renal parenchyma due to interstitial fibrosis can also result from repeated embolisms into the glomeruli from an atherosclerotic plaque that stenoses the renal artery.
The clinical picture in patients with ARH is associated with the development of several syndromes: • secondary hypertension, which is characterized by high levels of blood pressure (BP) with good subjective tolerability, refractory blood pressure to standard antihypertensive therapy; • renal failure (in 30–70% of patients), which is expressed in a decrease in glomerular filtration rate (GFR) and moderate azotemia (creatinine concentration in blood serum 130–400 µmol/l); • episodes of pulmonary edema of unknown origin (10%); • low back pain, which is associated with recurrent embolism from a stenotic plaque in the VA.
Diagnostics. Classic clinical and laboratory criteria for high risk of ARH are: • new hypertension (or its sharp worsening) in patients under 20 or over 50 years of age; • progressive hypertension in patients of any age; • combination of hypertension with signs of widespread atherosclerosis; • azotemia of unknown origin in combination with hypertension; • acute decrease in GFR and increase in azotemia (>30% of baseline) after the use of angiotensin-converting enzyme (ACE) inhibitors; • recurrent pulmonary edema in patients with uncontrolled hypertension; • the presence of systolic or systolic-diastolic murmur in the projection of the VA and abdominal aorta; • asymmetry in the size of the kidneys according to ultrasound examination (ultrasound), although a symmetrical decrease is possible with a bilateral process.
Diagnosis of VA stenosis is difficult, since the data from the anamnesis, physical examination and routine blood and urine tests are of low informative value for this pathology. If ARH is suspected, it is necessary to use special research methods.
Methods for diagnosing ARH: (1) functional tests: determination of plasma renin activity; determination of renin activity in the renal veins; dynamic renal scintigraphy during the use of ACE inhibitors; X-ray contrast angiography; (2) imaging methods: ultrasound (duplex scanning); magnetic resonance angiography; spiral computed tomography; X-ray contrast angiography.
Vasorenal hypertension
Kidney diseases provoke an increase in blood pressure. Vasorenal hypertension develops against the background of pyelonephritis, glomerulonephritis and chronic renal failure. This is due to the fact that excess fluid and salts are removed through the excretory system. If, due to kidney failure, this process is disrupted, water is retained in the body and provokes excess circulating blood volume and edema. Therefore, this type of hypertension and the pathology that provoked it are treated together.
Statistical data
Statistical observations show that renovascular hypertension can be detected in 5% of all individuals with high blood pressure with proper and high-quality examination.
Every fifth case of this form turns out to be resistant and does not respond to conventional drug therapy. In 1/3 of patients, a malignant course is observed with rapid progression of the disease and the development of complications.
Cases of hypertension among children under 10 years of age are especially alarming. 90% of them occur in altered renal arteries. In old age, this pathology is found in 42–54% of hypertensive patients, and among people with chronic renal failure - in 22%.
Experts consider these data to be underestimated due to poor quality examination of people with hypertension.
Causes of renovascular hypertension
Vasorenal conflict occurs against the background of such provoking factors:
- Atherosclerotic vascular lesions. With atherosclerosis of arteries and veins, the outflow of blood through them is disrupted due to narrowing of the lumen.
- Glomerulonephritis. This is an autoimmune or infectious lesion of the renal glomerulus, which results in disruption of the process of filtration and reabsorption of fluid.
- Fibromuscular dysplasia of the kidney. This disease is congenital, in some cases genetically determined.
- Pyelonephritis. This inflammatory disease of the renal calyces and pelvis leads to swelling of the organ parenchyma and blocking of the vascular lumens.
- Systemic vasculitis. This term refers to autoimmune lesions of the endothelial lining of blood vessels.
- Thrombosis of the renal veins. They appear due to the formation of blood clots in the systemic circulation.
- Malignant neoplasms. They block the vascular lumens and disrupt the process of fluid secretion from the body.
Chronic kidney disease is the most common cause of arterial hypertension of renal origin.
Causes
The causes of renovascular hypertension are as follows:
- the presence of atherosclerotic phenomena in the blood vessels of the kidneys. The formation of cholesterol plaques in blood vessels with a possible change in blood density or a tendency to narrow the lumen of blood vessels leads to a slowdown in blood flow in the kidneys:
- the presence of fibromuscular dysplasia, which manifests itself in the form of a gradual replacement of muscle tissue in the walls of blood vessels in the kidneys with scar tissue, which has less elasticity and is less restored after exposure. At the same time, a narrowing of the vessel also occurs with a deterioration in the quality of blood circulation in it. Externally, the affected part of the kidney artery looks like a rosary when thickening of the vessel and an aneurysm alternate. This pathological condition occurs most often in young girls;
- the development of nonspecific aortoareritis, in which the occurrence of an inflammatory process is noted. This condition is also called Takayasu's disease, in which arterial hypertension gradually intensifies and worsens, after the onset of which, after about 5-6 years, signs of renovascular hypertension begin to appear. At the initial stages of this process, there is a sclerotic change in only the inner side of the blood vessels of the kidney, but as the disease worsens, the entire vessel becomes sclerotic and is completely damaged.
Provoking factors of the disease include vascular sclerosis, which occurs after a series of irradiations during a treatment course for oncological diseases in the abdominal area (for example, with malignant tumors of the retroperitoneal region), dissecting aneurysm and stenosis of the renal arteries, into which the orifices of the renal vessels are gradually involved , peritoneal aortic embolism, compression of the renal aortic pedicle.
Diagnosis of the kidney condition should be carried out in cases of severely elevated blood pressure, as well as in the case of a hereditary predisposition to damage to the kidney tissue and blood vessels. This will allow timely identification of the current pathological process and eliminate the possibility of its aggravation.
How does the pathology manifest itself?
Vasorenal hypertension has the following clinical symptoms:
- Arterial hypertension. Systolic and diastolic pressure steadily increases.
- Edema syndrome. Swelling occurs throughout the body. The main localization is the face and lower extremities.
- Headache. It has a constant, pressing or bursting character. Painful sensations are localized in the occipital and parietal regions.
- Asthenic syndrome. It includes constant fatigue, weakness and depression.
- Unpleasant sensations in the lower back. They are caused by the enlarged kidneys stretching their own capsule, rich in nerve endings.
- Deterioration of vision. Patients complain of flashing spots or blurred vision.
- Dyspnea. It appears in the later stages, when arterial hypertension has time to negatively affect the state of the cardiovascular system.
Return to contents
Diagnosis of renovascular hypertension
A comprehensive study of the state of the cardiovascular and excretory systems is carried out. Arterial hypertension in case of renal dysfunction is diagnosed by the following laboratory and instrumental methods:
A urine test reveals elevated protein levels.
- General blood analysis. White blood cells increase slightly, erythrocyte sedimentation accelerates.
- General urine analysis. It shows an increase in protein secretion. With glomerulonephritis, intact or destroyed red blood cells are found.
- Biochemical analysis. The level of alanine aminotransferase and aspartate aminotransferase enzymes increases.
- Ultrasound of the abdominal organs. Indices of the ratio of the size of the kidney and blood vessels are calculated.
- CT or magnetic resonance angiography. A highly accurate technique helps to determine the percentage of reduction in the diameter of the vessel.
- Renal angiography. This is an x-ray method using a contrast agent. It helps to track the area where blood flow is impaired.
Return to contents
Diagnostic scheme
Experts suggest diagnosing renal artery stenosis sequentially in 3 stages. This will allow you to take into account the symptoms as much as possible and not miss the disease.
The first stage is to take into account the patient’s age, clinical features, frequent hypertensive crises, possible manifestations of acute heart failure, symptoms of chronic cerebral circulatory failure or encephalopathy. The examination determines:
- ECG shows signs of left ventricular hypertrophy with overload;
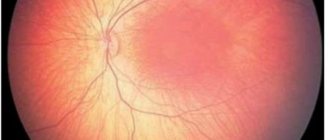
- in the fundus - retinal angiopathy;
- in urine analysis - increased secretion of protein and red blood cells;
- in biochemical tests - an increase in residual nitrogen and creatinine.
Using a photometer, the amount of protein in the urine is determined.
At the second stage, persons with identified pathology must undergo an instrumental examination. The most informative:
- ultrasound methods with Dopplerography of renal vessels;
- radioisotope renography or renal scintigraphy.
The diagnostic criteria are any identified asymmetric changes:
- in the size of the left and right kidneys;
- in the thickness of the cortical layer;
- in the structure of the vascular bed;
- in the secreting function.
At the third stage, the use of abdominal aortography is indicated. This method is by far the most reliable and allows for an accurate diagnosis in 99% of cases.
The given standard of step-by-step examination, according to experts, helps to reduce diagnostic time and avoid unnecessary costs for the patient and the medical institution.
X-ray after injection of a contrast agent into the abdominal aorta at the origin of the renal artery
Treatment of renovascular hypertension
Therapy for such a pathology should be carried out in conjunction with the relief of the disease that provoked it. For the treatment of renovascular hypertension, the following non-drug correction methods are used:
- Elimination of bad habits. The patient should give up smoking and alcohol abuse.
- Loss of body weight. Obesity is a provocateur of many diseases, including kidneys and blood vessels.
- Active lifestyle. Physical activity should be moderate but regular.
- Healthy eating. It is necessary to limit fatty and fried foods, foods high in sugar, stabilizers, preservatives, salt, dyes and flavor enhancers in the diet.
Return to contents
Drug treatment
For persistent increases in blood pressure, the following drugs are used:
- Angiotensin-converting enzyme inhibitors. These include Enalapril, Ramipril, Lisinopril and Captopril.
- Calcium channel blockers. These are the drugs "Verapamil" and "Nifedipine".
- Beta blockers. Among them are “Bisoprolol”, “Atenolol”, “Carvedilol”.
- Diuretics. The most commonly used are Furosemide and Veroshpiron.
- Statins. These medications reduce the risk of atherosclerosis. These include Atorvastatin, Simvastatin, Rosuvastatin.
Return to contents
Surgical intervention for renovascular hypertension
In severe cases, they resort to surgery. The principles of surgical treatment are to perform endovascular procedures and vascular reconstruction. Removal of the organ is less common. The first line is stenting or balloon angioplasty with stent placement. The second step is to remove the arteries through the kidney or aorta. The area is prosthetized or bypassed. In severe cases, nephrectomy is performed - removal of the affected kidney.
Recovery from renovascular hypertension
Hypertension leads to irreversible consequences. People who have had it should closely monitor their health and monitor their blood pressure daily. Such patients use antihypertensive medications and diuretics for life. To improve their condition, patients use a special diet and engage in moderate exercise. Compliance with all these preventive measures will help avoid serious complications such as stroke and heart attack.
Symptoms of vasorenal arterial hypertension
The disease does not have any specific symptoms; they may vary depending on the stage of development of the pathology. However, there are some manifestations that occur in the vast majority of cases. These include:
- Regular headaches;
- Ringing in the ears, flickering of “flies” before the eyes;
- Sleep disturbance (insomnia);
- Feeling of chest tightness;
- Heart rhythm disturbances;
- Pain in the lumbar region;
- Frequent urination;
- Increased thirst.
The disease in all cases is accompanied by high blood pressure, sometimes not amenable to drug therapy. Most often, it is possible to lower the levels only after the main cause of renovascular hypertension has been eliminated.