Percutaneous angioplasty is hope for myocardial infarction.
The article will talk about a minimally invasive surgical intervention called angioplasty, which has been widely used in recent years. It will be discussed what kind of procedure this is, in what cases it can be used in cardiac patients, and, conversely, what contraindications it has for its use.
Features of its implementation, positive and negative aspects when choosing this method, as well as the course of the postoperative period - all these issues will be discussed in this article.
Angioplasty of cardiac vessels is the main treatment option today, both for myocardial infarction and for coronary heart disease in the form of stable angina, if indicated. This method has received the greatest development in recent years thanks to various scientific studies conducted on this topic.
General information
The historical beginning of the development of angioplasty as a separate direction not only in cardiology, but also in vascular surgery in other areas was laid back in 1964. Since that moment, not only this method of treating stenotic vessels has undergone rapid development, but also other directions have emerged in solving the problem of arterial occlusion of both the coronary pool and the arterial bed of other areas.
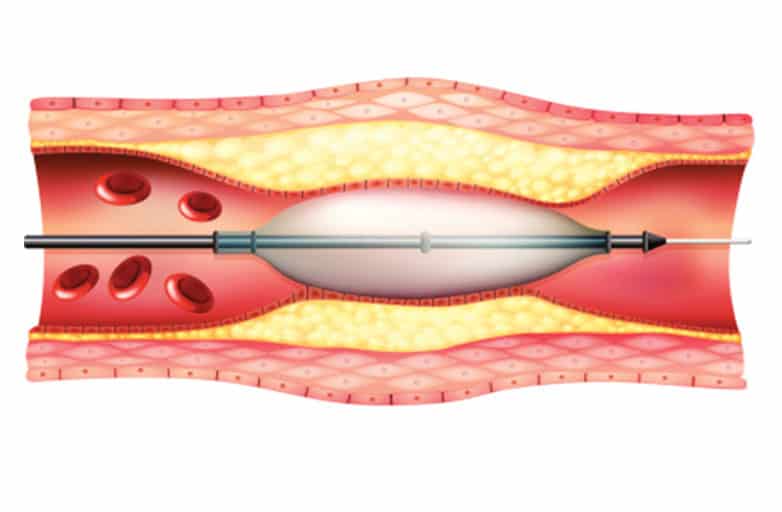
The principle of operation of this method is based on increasing the lumen of a vessel affected, for example, by atherosclerosis, by installing a foreign stent at the site of the plaque, opening it with the help of special balloon devices, allowing the stent to acquire the shape and suitable diameter of the vessel. As a result, the blood flow disturbed in this area is resumed and leads to normalization of the perfusion of the myocardial area, muscle skeletal tissue or brain, etc.
The photo shows a still unopened wall in the lumen of the vessel.
Despite the “ideality” of the invented revascularization method, there are a number of undesirable complications, contraindications for its implementation and, in particular, strict indications. This will be discussed later.
Secrets of the angioplasty procedure
Despite the fact that cardiac angioplasty has a superficial resemblance to coronary angiography due to the fact that the same access is used, and in general angioplasty is a continuation of simple angiography, it carries a higher risk. Manipulation aimed at highly selective catheterization of a known diseased vessel has a risk of undesirable complications of 1%, while angiography of the coronary arteries is 0.1%.
Potential complications are influenced by factors such as the patient's overall condition, the choice of angioplasty technique, the severity of the vessel occlusion and the ability to gain access to it.
Angioplasty is performed by an interventional cardiologist.
Important! Possible complications are rare, but possible, so the doctor performing the procedure usually informs both the patient and his family about them.
Angioplasty is performed in highly specialized centers that have access to a team of cardiac surgeons and anesthesiologists necessary for complications. The only exception in which the complete absence of a cardiac surgery team in the clinic at the time of the revascularization procedure is possible is acute myocardial infarction with ST interval elevation above the isoline (STEMI).
If we talk about elective angioplasty, the patient usually comes to the clinic in the morning of the same day when the procedure is scheduled, or the day before the designated date, to conduct a full range of studies necessary for the preoperative preparation of the patient. Be sure to read to the end of this article to find out everything why cardiac angioplasty is performed.
Next, we will consider the features of preoperative preparation of the patient.
- On an empty stomach. Liquid and food intake should be stopped at least 6-8 hours before the start. The exception is small amounts of clear water if necessary and in order to wash down medications.
- Drug therapy. Prescribing Aspirin in a large dose before the procedure is necessary to reduce platelet aggregation on the already damaged endothelium of the coronary arteries. This helps to facilitate stent placement during the procedure. For patients suffering from hypersensitivity reactions to acetylsalicylic acid, it is necessary to use a desensitization protocol before or immediately after angioplasty. A drug such as Clopidogrel, which belongs to the group of antagonists of specific ADP receptors, can be used before the procedure, which also helps prevent platelet aggregation among themselves. Its effect can be enhanced by taking glycoprotein IIb/IIIa inhibitors, which can significantly reduce the risk of acute myocardial infarction during the procedure and shortly after it.
- Allergy to iodine. It is worth considering the fact that a patient who is prescribed cardiac vascular surgery may have a hypersensitivity reaction to drugs containing iodine. The latter is used as a contrast in this procedure. For such cases, there is a protocol of necessary measures aimed at desensitizing the patient’s body and reducing the risk of developing an immediate allergic reaction.
Depending on the patient's peripheral vasculature and the provider's skill and preference, vascular access is usually through the femoral, radial, or brachial arteries. The first two are the leaders in frequency.
A catheter used to provide arterial access.
Standard angioplasty does not require catheterization of the right half of the heart, however, if the patient assigned to this procedure has initial hemodynamic disturbances, additional venous access and placement of a catheter in the right half of the heart can be used. This allows you to obtain the most accurate data on the patient’s hemodynamics in real time, and, if necessary, perform stimulation. This is discussed in more detail in the video in this article.
After arterial access has been established and a conductive sheath has been installed in it, through which catheters will subsequently be advanced towards the heart, antithrombin therapy is usually carried out using unfractionated heparins. As an alternative, drugs of a number of low molecular weight heparins or direct thrombin antagonists can be used. The choice of therapy lies with the attending physician.
The use of any of the above groups has its own characteristics. Instructions for antithrombotic therapy may require dosage reduction in some cases, repeated administration of the drug, or monitoring the effect of drugs using laboratory diagnostics.
The primary angiogram visualizes the right coronary artery.
After this, the catheter is inserted directly into the sinuses of the coronary arteries located near the aortic valve leaflets. This allows a baseline angiogram of the left and right coronary arteries to be obtained.
The reasons for performing an initial angiogram are as follows:
- assessment of possible changes in the vessels over the period of time from the previous angiography, if any;
- selection of appropriate angles for viewing the stenosis, which is necessary for complete visualization during angioplasty;
- planning a detailed intervention strategy for this particular patient.
Selective angiography of the left coronary artery.
Attention! Intracoronary administration of nitroglycerin makes it possible to determine the organic nature of the existing occlusion in the vessel to exclude spasm as the cause of angina.
Depending on the extent of damage in the vessel, the focus of the heart muscle suffering from reduced perfusion due to the presence of occlusion in the coronary artery, the approach to revascularization is determined in each specific case, and the choice of device for opening the vessel. In this case, the size of the stenosis and the diameter of the lumen are compared with the diameter of the catheter used.
Using contrast, the exact location of the stenosis is determined and a catheter with a balloon is advanced directly to the site of occlusion. Only after it is confirmed that the device is in the correct location, the balloon is inflated, thereby forming a site for the subsequent installation of the stent selected by the doctor.
Schematic illustration of balloon angioplasty.
Important! The lumen of the balloon contains not air, but a contrast agent, which makes it possible to better assess the location of the catheter, as well as prevent air embolism in the distal branches of an already affected coronary vessel.
Today, there are stents that do not require prior balloon dilatation; however, even in the case of such direct stenting, expansion of the balloon at the site of vessel occlusion allows subsequent stent placement more quickly, safely, and accurately.
A stent used in a percutaneous angioplasty procedure.
After preparing the vascular base for stent installation, depending on the obtained diameter of the artery lumen, the corresponding diameter of the stent used is selected. This is carried out by a specialist in interventional cardiology.
Selecting a suitable stent is a complex and at the same time important task. If the stent is in the wrong position relative to the location of the stenosis, or does not fit in length, thereby not opening the artery completely, it is impossible to remove it after complete installation.
Important! The stent is also placed on a balloon, which allows it to be deployed to fully open the coronary artery.
Previously, the revascularization method with isolated balloon angioplasty was used, but today cardiologists are guided by the following rule: “Any damage that can be stented must be stented.” Undoubtedly, there are exceptions to every rule, and interventional cardiology only confirms this fact.
The process of opening a coronary artery and installing a stent.
After installation of the stent, the procedure does not end, and further manipulations are aimed at the effectiveness of the revascularization performed. So, in addition to introducing a contrast agent directly at the site of installation of the device to determine blood flow through the vessel, the calculation of the trans-stenotic pressure gradient, or the use of adenosine for artificially induced vasodilation, is used.
Once adequate dilatation of the damaged vessel has been confirmed, the devices used in the angioplasty process are removed and the arterial access is closed. For the latter, it may take time to stop the bleeding (for the femoral artery, prolonged compression of the puncture site is sometimes necessary).
Possible risks of coronary angioplasty
Although angioplasty is less invasive than bypass surgery, the procedure still carries some risks. Risks may be associated with the procedure itself and its long-term outcomes.
Early risks:
- Bleeding. There may be bleeding in the leg or arm where the vessel was accessed. Usually it just develops as a bruise, but sometimes there is serious bleeding that may require a blood transfusion or surgery.
- Heart attack. Coronary circulation disorders develop very rarely during surgery, but sometimes, due to technical reasons, a rupture or dissection of the coronary artery may develop. These complications may require emergency coronary artery bypass surgery.
- Kidney problems. The contrast agent used in angioplasty and stent placement can cause kidney damage, especially in people who already have kidney problems. If you are at higher risk, your doctor may take steps to protect your kidneys, such as limiting the amount of contrast material and increasing fluid intake to dilute the contrast.
- Ischemic stroke. During angioplasty, a stroke can occur if pieces of plaque break off as the catheter is passed through the aorta. Stroke is an extremely rare complication of coronary angioplasty. To prevent it, drugs that reduce blood clotting are prescribed.
- Heart arythmy. During the procedure, the heart may beat too fast or too slow. Such arrhythmias are usually short-lived, but sometimes a temporary pacemaker is required.
Late complications
- Repeated narrowing of the artery (restenosis). With angioplasty without stenting, the rate of restenosis is approximately 30% of cases. Stents have been developed to reduce restenosis. The use of plain metal stents reduces the risk of restenosis to 15%, and the use of drug-eluting stents reduces the risk to less than 10%.
- Stent thrombosis. Blood clots (thrombi) can block an artery, causing a heart attack. To reduce the risk of thrombosis, it is important to take aspirin, clopidogrel (Plavix), which helps reduce the risk of blood clots forming in the stent. Never stop taking these medications without talking to your doctor.
Patient management after the procedure
Thanks to the recently widespread special devices that close the puncture in the artery, removal of the conductor sheath installed at the arterial access site is possible immediately after the end of the manipulation. After this, the patient remains in bed for an average of 18 to 24 hours without complications.
Percutaneous angioplasty is usually performed simultaneously by two cardiologists.
If a glycoprotein IIb/IIIa blocker was administered to the patient during the procedure, it continues to be given for another 18 hours after the end of the angioplasty.
Aspirin and Clopidogrel are also given to the patient after surgery, and the duration of treatment and dosage of the latter varies depending on the type of stent used. So, when installing a metal stent, taking Clopidogrel continues for up to 2-4 weeks, and if a drug-coated stent was installed, taking this drug is extended for a period of 3 to 6 months.
Important! The absence of symptoms of myocardial ischemia is expected immediately after stent placement.
Stages of balloon angioplasty:
Of course, like any other procedure, this operation consists of several stages, where each of them is interconnected.
• Artery puncture.
• Injection of a radiopaque solution into the artery to examine its lumen.
• Passing a special guide through the area of narrowing, in other words, blockage of the artery.
• Delivery of the balloon catheter to the desired area and inflation of the balloon.
• Repeated injection of a radiopaque solution into the artery to evaluate the result of balloon angioplasty.
• Removing instruments from the artery, also applying hemostasis.
Balloon angioplasty of the lower extremities at Barzilai
The specialists of our clinic have all the professional skills and knowledge for this, as well as enormous experience in such operations. After it is performed, our patients are usually discharged from the hospital the next day after the bandage is removed, as they can already begin their usual routine of life. It is not without reason that balloon angnoplasty is most often called surgical treatment without surgery, since after it is performed, patients are left with no trace of stitches or scars.
Continuous improvement of the endovascular instrument and the expanded experience of our staff in performing these surgical interventions allows us to effectively restore blood flow in all areas of the arterial vessels of the lower extremities, from the large iliac arteries to the small arteries of the foot. We also perform a combined operation, combining all the advantages of both methods, especially if we are talking about a severe case of damage to the vessels of the limb. Contact us and we, with our wealth of knowledge and experience, will make every effort to ensure that balloon angioplasty of the lower extremities
passed with the greatest effectiveness and with the least likelihood of injuries.
Indications and contraindications for use
Having recently become the most popular and effective treatment for myocardial infarction, being the best alternative to bypass surgery and drug therapy, its use is still limited by a number of strict indications.
This:
- Asymptomatic ischemia. This group includes patients with one or two affected coronary arteries and instrumentally and laboratory-confirmed ischemia of the heart muscle.
Attention! The asymptomatic course of myocardial ischemia and myocardial infarction, in particular, is most typical for patients with diabetes mellitus.
- Unstable angina or stable moderate angina. Stable angina, the symptoms of which classify it as class II-IV in severity, or unstable angina require not only angiography, but also angioplasty.
- STEMI. Myocardial infarction with ST segment elevation above the baseline is a “red flag” that requires urgent treatment, the most effective of which is cardiac angioplasty. In this case, the individual characteristics of both the patient himself and his condition at the time of the infarction and the extent of necrosis play an important role in the choice of this method.
- Previous bypass surgery. Patients with a history of early bypass surgery who present to the hospital with symptoms of angina pectoris should be considered candidates for angioplasty.
Theoretically, repeat bypass surgery is possible, but it carries a high risk of adverse complications.
For chest pain, consultation with a cardiologist is required.
Contraindications for angioplasty
The main situations in which this type of therapy for myocardial ischemia is not used are the following:
- occlusion of a vessel whose diameter is reduced by less than 50% of the proper lumen;
- stenosis of the main trunk of the left coronary artery;
- clinically significant occlusion of three or more coronary arteries.
The last two factors are indications for referring the patient to open surgery - bypass surgery.
Other contraindications include certain health conditions of the patient, such as impaired blood clotting, congestive heart failure in the decompensation stage, renal failure, acute cerebrovascular accident, etc.
Types of angioplasty surgery
The most popular types of angioplasty include:
- Reconstruction of arteries clogged with atherosclerotic plaques. Stenting the arteries of the lower extremities, usually the iliac artery, prevents surgery that directs blood flow around the blocked aorta, iliac arteries through an artificial vessel. This operation is performed by highly professional vascular surgeons. Aortofemoral replacement is recognized as a meticulous surgical method aimed at restoring blood flow due to blockage of the iliac arteries. Atherosclerotic lesions of the iliac artery are observed in most patients with arterial pathologies of the lower extremities. Treatment methods for severe narrowing of the iliac artery are balloon angioplasty or stenting.
- Surgery of the superficial femoral artery. Surgical procedures involve strengthening the wall of a stretched artery with a stent that looks like a mesh. The procedure is designed to eliminate the phenomena of chronic arterial insufficiency in case of blockage of the vessel cavity.
- Surgery of the iliac artery. Medical observations determine this operation to be the most popular among other types of angioplasty. Balloon angioplasty has shown excellent results in the treatment of severe narrowing of the arterial cavity. Balloon angioplasty is painless and is performed under local anesthesia.
- Balloon angioplasty, which provides additional coverage. This technique involves immersing a balloon in a special medicine and then saturating its surface. When the balloon enters the arterial cavity, the medicine exerts its therapeutic effect. This reduces the focus of inflammation and prevents subsequent progression of the disease.
Balloon angioplasty of the legs is indicated for serious clinical cases when immediate healing of purulent wounds of various etiologies is required. A sequence of coordinated actions by surgeons can stop tissue necrosis in the diabetic foot. The expansion of the lumen of the arterial cavity of the lower extremities remains in half of the operated patients.
At first glance, the procedure is wonderful, but many patients are alarmed by the question even at the initial visit to the doctor: who exactly is the operation suitable for? What restrictions will become an obstacle to surgical intervention?
Medical experts state that a patient may be prohibited from undergoing such surgical intervention if the patient himself disagrees, as well as if there is:
- symptoms of infectious damage to the body;
- high blood pressure;
- failure of the hemocoagulation system;
- abnormalities in the functioning of the liver organs;
- inability of the cardiovascular system to supply tissues and organs with blood in the required quantities;
- period of regression of chronic diseases;
- acute pulmonary failure;
- inflammation of the endocardium.
In addition to all that has been said, a parallel can be drawn between conservative surgery and angioplasty.
Questions for the doctor
It's a question of time
Hello, my name is David. I suffer from stable angina, but over the past three months I have developed severe chest pain, which occurs at a time when I do not expect it, in a situation that is not at all stressful for me. An example would be the pain two weeks ago that woke me up and was only able to fall asleep after taking two nitroglycerin tablets. Tell me, please, should I see a doctor or is this the normal course of my illness?
Good afternoon, David. The symptoms you describe are characteristic of progression of the disease to episodes of unstable angina.
Even one such episode is a direct indication for consultation with a specialist and conducting a series of instrumental and laboratory studies in order to clarify the extent of the process and resolve the issue of necessary therapy in your case.
You should not postpone the process of going to the doctor until another “unexpected” episode of pain occurs. The cost of timely treatment and initiation of therapy is directly proportional to its effectiveness.
Possible complications
It has been proven that the transluminal procedure can have the following complications:
- a hematoma forms in the puncture area;
- an allergy to the contrast agent may occur;
- serious changes in heart rhythm occur;
- thrombosis occurs.
Patients rarely experience such conditions, but if problems arise, the patient should receive immediate medical attention. Angioplasty with stenting is considered the safest method of eliminating vascular atherosclerosis and treating coronary heart disease.
With balloon angioplasty, the mortality rate among patients with vascular disease is greatly reduced. But for unstable angina, balloon angioplasty exposes the patient to a greater risk of complications.
Stable angina has fewer such cases. Previously, it was difficult for doctors to determine how many segments of the vessel were affected, so coronary artery angioplasty did not help patients as often as it does today.