Heart valve defects
Heart valve defects: description
When a valve cannot close properly (valvular insufficiency) or does not open completely due to certain diseases, obstructing the flow of blood (valvular stenosis), then we can talk about a disease called “heart valve defects”. Depending on the severity of the disease and on its basis, heart failure with corresponding symptoms may develop gradually or in an acute form. The following types of heart valve diseases are distinguished: valvular stenosis (aortic stenosis, stenosis of the mitral valve, pulmonary artery, tricuspid valve), as well as valvular insufficiency of the aorta, mitral valve, pulmonary artery, tricuspid valve.
Heart valve defects : symptoms
According to the New York Heart Association (NYHA) classification, symptoms of valve diseases are divided according to the severity of functional disorders of the cardiovascular system into four main groups. Mild and moderate forms of valvular insufficiency often do not cause any symptoms.
A classic sign of the disease is decreased performance during physical activity. These include: shortness of breath, rapid pulse, arrhythmia, fatigue, and sometimes dizziness. If the valves on the left side of the heart (aortic or mitral) are not able to fully move blood, then it is thrown back into the pulmonary vessels, and excess fluid seeps through the capillaries into the alveoli, causing difficulty breathing (shortness of breath).
In severe cases of aortic stenosis, in addition to shortness of breath, angina, dizziness and fainting may occur. If there are valve defects on the right side of the heart (tricuspid or pulmonary valve), then symptoms of right-sided heart failure appear, namely: accumulation of fluid in the abdominal cavity (ascites), the appearance of edema in the legs and ankles.
Heart valve defects: causes and risks
The main causes of acquired heart valve insufficiency are:
rheumatism or inflammation of the connective tissues of the mitral and aortic valves;
degenerative changes in heart valves (eg, calcification, prolapse, Marfan syndrome);
infectious diseases of the heart muscle: endocarditis, myocarditis, or both;
complications after cardiac diseases (post-infarction condition, excessive expansion of valves as a result of pulmonary hypertension).
Heart valve defects: examination and diagnosis
To determine the severity of the disease, along with a basic medical examination, diagnostic procedures such as echocardiography and, in some cases, MRI or cardiac catheterization are performed. A more complete picture of the morphology of the heart valves can be obtained using transesophageal echocardiography. In this procedure, an ultrasound probe is inserted down the throat into the esophagus, which is located close to the heart, and sound waves help to see a clear image of the myocardium on a monitor. Currently, the latest diagnostic methods are often used, especially before surgery, such as 3D echocardiography and 3D Doppler color imaging. Traditional methods for studying heart valve diseases include ECG, as well as continuous Holter monitoring of a long-term ECG procedure.
Heart valve defects : treatment
The basis of heart valve insufficiency is usually a mechanical problem that cannot be treated with medication. The only exceptions are acute infectious diseases of the heart valves, for example, infective endocarditis, in which the further development of valvular insufficiency can only be stopped with the help of a large dose of antibiotics.
With the help of drug therapy, the discomfort caused by a defective heart valve can be eliminated. For example, for shortness of breath, diuretics (diuretics) are used; when the pumping function of the heart muscle is weakened and the size of the atria increases, ACE inhibitors, AT antagonists and beta blockers are used; To slow the heart rate during atrial fibrillation, drugs such as beta blockers or verapamil, drugs from the glycoside group are prescribed, and to prevent thromboembolism, anticoagulants with a vitamin K antagonist are additionally used.
Surgical correction of valvular insufficiency involves either reconstruction or replacement of the valves. Mitral valve reconstruction is one of the most common operations. A new non-surgical treatment method, the percutaneous MitraClip® procedure, is now recognized and approved for clinical use as an effective treatment for mitral valve disease. It is especially successfully used in the treatment of frequently occurring functional mitral valve insufficiency. The MitraClip method is an important therapeutic option for selected high-risk patients with congestive heart failure.
The heart valve can be replaced surgically with either a mechanical one or a prosthetic one made from biological material.
An alternative to open-heart surgery to replace the aortic valve is percutaneous transcatheter implantation of its bioprosthesis (transcatheter aortic valve implantation, TAVI). Placed in a rolled metal mesh and secured to the end of the catheter, the prosthetic heart valve is advanced through the vascular system transarterially—usually through the femoral artery—or transapically—directly into the heart cavity, to the aortic valve, where it is positioned and deployed.
Heart valve defects: course of the disease and prognosis
The prognosis for heart valve insufficiency depends, first of all, on which valve is affected, as well as on the degree of damage to the heart muscle. Advanced disease can lead over time to myocardial weakness and ultimately death. Mild forms of valvular insufficiency are usually not subject to surgical intervention and are not life-threatening.
Heart valve defects: other comments
If a patient has a mechanical heart valve, careful monitoring of the anticoagulation process (inhibition of blood clotting) and timely administration of the prescribed dose of the appropriate drug (anticoagulant) is necessary.
mechanical and biological prostheses are more prone to bacterial infections than your own heart valves, especially if bacteria grow in the blood. In this regard, for patients who have biological or mechanical valve prostheses, or who have undergone valve reconstruction surgery using synthetic materials, in the presence of a bacterial infection, for example, purulent bronchitis, purulent inflammation of the paranasal sinuses, or infections of the urinary system, treatment with antibiotics is recommended.
Source: ims.uniklinik-freiburg.de
Statistics
The disease is common in all countries of the world and in different climate zones. The incidence ranges from 3.1 to 11.6 per 100,000 inhabitants . Men suffer from endocarditis 2–3 times more often than women.
Recently, in developed countries this pathology has been reported. If previously the average age of patients with endocarditis was 35 years, now it is 50. The risk of developing the disease in early childhood is also higher, especially in the presence of congenital heart defects.
Prevalence
In developed countries, coronary heart disease has become the most common cause of death and disability, accounting for about 30 percent of deaths. It is far ahead of other diseases as a cause of sudden death and occurs in one in three women and half of men. This difference is due to the fact that female sex hormones are one of the means of protection against atherosclerotic vascular damage. Due to changes in hormonal levels during menopause, the likelihood of a heart attack in women after menopause increases significantly.
Kinds
The division into types of disease is made on the basis of the reasons that caused it. Conventionally, they are divided into two large groups: aseptic and bacterial inflammation.
The first group includes rheumatic, Libman-Sachs and Leffler. The second is diagnosed much more often; it includes a bacterial or septic and infectious process.
- Infectious (bacterial) endocarditis (ICD code I33.0 or I33.9) occurs when the outer lining of the heart is damaged by streptococci, staphylococci or fungi. Develops with tuberculosis, syphilis and brucellosis. The main cause of development is the entry of viridans streptococcus into the heart tissue. But against the background of a weakened immune system, the disease can be provoked by pneumococcus, enterococcus and E. coli.
- Septic (ICD-10 code I33.0 or I33.9) develops against the background of sepsis. The cause is gram-positive cocci. In 80% of cases, the disease is secondary and occurs in patients with rheumatic, less often syphilitic, atherosclerotic or congenital heart disease.
- Rheumatic endocarditis (ICD-10 code I01.1). The aseptic process occurs without the participation of pathogenic microorganisms. It is a concomitant disease in rheumatic, allergic diseases and autoimmune conditions.
- Loeffler's endocarditis (ICD-10 code I42.3) is otherwise called endomyocardial (eosinophilic) disease. The cause of the pathology is an increase in the number of eosinophils. These cells accumulate in the heart muscle and cause specific inflammation. This condition occurs as a result of autoimmune disorders, allergic and parasitic diseases, and cancer.
- Liebman-Sachs endocarditis (ICD-10 code I39* M32.1) is observed in systemic lupus erythematosus. In this pathological condition, patients develop antibodies against their own body, resulting in swelling and inflammatory processes.
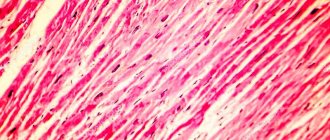
Progress and diagnosis of inflammation of the heart muscle
Myocarditis can be fulminant, acute, subacute or chronic. In the case of lightning-fast progression of the disease, there is a rapid increase in cardiac symptoms. This can lead to cardiogenic shock , that is, a group of symptoms associated with acute hypoxia of key organs, in a relatively short time. The fulminant form of myocardial dysfunction ends either in self-healing or in the death of a person.
Acute inflammation of the heart muscle is characterized by less defined initial cardiac symptoms, a slow increase in their intensity and a high likelihood of developing complications, in particular dilated cardiomyopathy.
Chronic myocarditis has symptoms similar to dilated cardiomyopathy - enlargement of the heart chambers, impaired active contractions, and, consequently, heart failure, which progresses. If dilated cardiomyopathy develops, the chance of survival for the next five years without appropriate treatment is 50%.
The worst prognosis occurs in patients with chronic or subacute myocarditis. This form of the disease is often associated with the constant presence of a virus in the heart muscle, which the body is unable to fight, and the chronic inflammatory process contributes to the gradual and progressive degradation of the heart. Because antiviral antibodies, in addition to destroying the virus itself, destroy the proteins of the heart muscle. The breakdown of infected cells in the heart causes further production of antibodies. This leads to the formation of a vicious circle, resulting in damage to the heart that prevents its further functioning.
The best prognosis is given by asymptomatic myocarditis, which on the ECG resembles a “fresh” myocardial infarction. In such cases, differentiation occurs on the basis of coronary angiography, that is, x-rays of the arteries of the heart with contrast. The correct image of the arteries indicates a mild form of myocarditis, during which, if the disease does not worsen, contractility disorders usually disappear spontaneously and the patient gets better.
In addition, the majority of patients affected by fulminant or acute forms of inflammation of the heart muscle recover, as a rule, after removal of the infection that causes myocarditis, unless sudden death occurs during the course of the disease. However, the heart of a person who has suffered a fulminant or acute form of myocarditis does not return to full health.
It is especially difficult for people who smoke cigarettes. They have a higher mortality rate and an increased risk of heart attack during inflammation. Also, individuals who use certain drugs, especially cocaine, are at risk of severe disease.
To accurately find and recognize the disease, studies such as:
- blood tests - an increased sedimentation rate can be observed in most patients. The morphological picture shows leukocytosis, that is, an increased number of white blood cells - leukocytes, usually with a predominance of neutrophils. If the cause of myocarditis is an infection, eosinophilia, that is, an increased concentration of eosinophils, will naturally be detected.
- electrocardiography - the ECG image in patients with inflammation of the heart muscle is usually abnormal: arrhythmia, conduction disturbances and other changes are visible.
- echocardiography - used mainly to diagnose fulminant inflammation of the heart muscle. In this case, normal diastolic volume is visible, but also a significant deterioration in contractility and thickening of the wall of the left ventricle.
- X-ray examination - shows cardiomegaly, which is associated with a more advanced stage of inflammation of the heart muscle. In addition, if there is a circulatory disorder, fluid may be visible in both lungs.
- magnetic resonance - allows you to detect a heart tumor and localize the source of inflammation, which can facilitate diagnosis and biopsy.
- endomyocardial biopsy - a fragment of myocardial tissue is obtained in order to detect possible necrosis of cardiomyocytes and inflammation. However, a biopsy does not always detect existing inflammation in the heart area, so a negative result does not mean the absence of inflammation.
Etiology: causes and risk factors
- Rheumatism.
In rheumatism, the leading etiological agent is group A beta-hemolytic streptococcus, which penetrates the cardiac structures through the bloodstream.
Having a structure similar to the connective tissue membranes of this hollow muscular organ, it provokes a false immune response, resulting in damage to the mitral, tricuspid and aortic valves, and rheumatic pathology occurs.
- Infection.
Among microbial factors, the main role is given to bacteria - gram-positive pathogenic flora: streptococci, in particular group D streptococci and enterococci, as well as staphylococci and pneumococci.
Pathogens from the group of gram-negative rods are much less common. Salmonella, Legionella, Shigella and Pseudomonas are especially pathogenic.
The fungal form is also an uncommon occurrence: as a rule, it occurs as a complication of long-term antibiotic therapy in the postoperative period or to prevent secondary infection when vascular catheters are installed.
- Injuries and operations.
Surgical interventions, diagnostic and therapeutic invasive procedures (catheterization of central veins, colonoscopy and cystoscopy, parenteral administration of drugs, hemodialysis, etc.) create an entrance gate for the penetration of pathogenic microorganisms into the vascular bed that can cause inflammation.
Among the predisposing factors for the development of endocarditis are:
- hidden foci of dormant infection of various locations: tonsillitis, carious teeth;
- congenital and acquired heart defects, hereditary anomalies of its development;
- primary and secondary immunodeficiency;
- stress, sluggish chronic diseases that weaken the body’s defenses;
- addiction;
- elderly age.
Learn more about this disease from the video:
Classification
According to the nature of the flow
Here they highlight:
- primary : occurs on healthy heart valves;
- secondary : develops on pathologically altered structures of the heart and blood vessels during rheumatism, congenital and acquired defects, syphilis, after surgery for valve replacement, etc.
According to the clinical course there are:
- acute : lasts up to 2 months.
The reason is sepsis of staphylococcal origin, trauma and therapeutic and diagnostic manipulations in the field of the cardiovascular system. With this form of inflammation, infectious and toxic manifestations rapidly increase, as well as valve vegetation and thrombus formation, and purulent metastases to various organs are not uncommon; - subacute : lasts more than 2 months. Develops with inadequate treatment of acute endocarditis;
- chronic recurrent : more than 6 months. Formed with deep damage to the myocardium or dysfunction of the valve apparatus. It is more common in newborns and infants with hereditary heart defects, drug addicts and people who have undergone surgical interventions.
Stages
There are three stages of the pathogenesis of endocarditis: infectious-toxic, immunoinflammatory and dystrophic.
- First stage begins with the entry of a pathogenic agent into the bloodstream, which causes damage to the valvular and parietal endocardium. Ulcerations appear on the inner membrane. On the affected areas, growths of fibrin strands and platelets begin to form.
Then bacteria attach to the vegetation, and secondary septic foci of infection are formed. Blood clots breaking away from the walls cause thromboembolic complications.In addition, along with severed vegetations, bacteria are spread throughout the body, which settle in various organs and cause inflammatory processes in them.
- The immunoinflammatory stage begins with immune generalization of the process.
At this time, the body begins to produce antibodies not only against bacteria, but also against its own tissues, and autoimmune conditions develop. A clinical picture of extensive damage to internal organs develops. Characteristic of this phase is glomerulonephritis and arthritis of large joints, and with a long course of the process - splenomegaly (enlarged spleen). - During the third stage , against the background of sepsis and increasing heart failure, irreversible dystrophic changes appear in many organs. Failure of internal organs (renal, liver, etc.) is added to the existing disease; in severe cases, myocardial necrosis develops.
By localization
According to the localization of endocarditis, they are distinguished:
- left-sided inflammation of the native (natural) valve;
- left-sided endocarditis of the prosthetic valve, which is divided into early (less than a year after installation) and late (more than a year has passed since the operation);
- right-sided endocarditis;
- associated with devices such as a pacemaker.
In addition, valvular, parietal and chordal pathologies are distinguished.
When a disease develops on the valve apparatus, only the leaflets may be involved in the process (valvulitis), which is more common in the rheumatic process. While the infectious variety covers all parts of the valve: leaflets, valve ring, chords and papillary muscles.
In the acute septic form of the disease, the mitral valve is affected, in the subacute form - the aortic valve, and chronic sepsis causes isolated inflammation of the tricuspid valve. Gradually, inflammation spreads from the valves to the parietal endocardium and chordae tendineae.
Aortic regurgitation, causes, symptoms, treatment
Aortic regurgitation is caused by aortic dissection or serious injury. The chronic form of the pathology is caused by a history of endocarditis, which occurred in an infectious form. Sometimes the aortic root can expand, degenerative processes occur in the body, rheumatic fever.
The main clinical signs include:
- severe pain in the lungs, swelling, shortness of breath,
- in the area of the lower edge of the sternum on the left side, a protodiastolic murmur is clearly audible,
- increased heart rate,
- displacement of the upper part of the heart because there is strain and pressure on the left ventricle.
In the acute form of development, patients experience a sharp deterioration in well-being. They need urgent help. In this condition, pulmonary edema often occurs, which has a high probability of death.
After the examination, the doctor decides on the advisability of emergency valve replacement. The patient is provided with appropriate treatment to maintain the body. The patient is prescribed diuretics, vasodilators, and inotropes.
Clinical picture: main signs
The clinical picture of the disease is individual in each case, but there are also general manifestations of endocarditis. Most patients experience a slow progression of the disease. The subacute process can last up to several months . In this case, the signs are smoothed out. In the case of an acute process, obvious symptoms of the disease are observed.
For a long time (more than 10 days), the patient experiences an increase in temperature above 38 degrees, sweating and chills. During this period, weight loss occurs. Intoxication gradually develops, as evidenced by weakness, loss of appetite, headaches, and insomnia.
After some time, the temperature drops, and pain in the heart area and shortness of breath appear. Due to increasing intoxication, the elasticity of the walls of blood vessels is impaired. Minor hemorrhages appear on the skin and mucous membranes. With a long process, pronounced signs appear: fingers become like drumsticks, and nails become like watch glasses .
Symptoms
Signs of inflammation of the heart muscle depend on the cause and severity of the disease. For example, many people with myocarditis caused by the Coxsackie virus do not have any symptoms of the disease. The only indicator of inflammation in the heart muscle may be a temporary abnormal result on an electrocardiogram (ECG), a test that measures the electrical activity of the heart. Or, when conducting echocardiography (ultrasound examination of the heart), some changes may be detected, for example, reduced contractile activity of the myocardium.
Typical symptoms of inflammation of the heart muscle include chest pain and arrhythmia, which occur during or shortly after an infection. In most cases, myocardial damage is mild, heals quickly and completely, and does not affect the pumping function of the heart. However, inflammation of the heart muscle can sometimes cause extensive damage, leading to myocardial failure. This life-threatening condition requires prompt care in a specialized facility. Fortunately, this condition is quite rare.
Common symptoms of inflammation of the heart muscle in adults include:
- chest pain;
- arrhythmia (abnormally fast, slow, or irregular heartbeat);
- sudden loss of consciousness (fainting);
- temperature increase;
- pain and swelling in the joints;
- signs of heart failure (shortness of breath, swelling of the legs);
- fatigue.
A child with myocarditis may have the following signs:
- temperature increase;
- tachycardia or arrhythmia;
- rapid breathing;
- difficulty breathing, especially when moving;
- the appearance of anxiety or irritability;
- poor sleep;
- refusal to eat;
- increased sweating;
- weakness, lethargy, apathy, fainting;
- rare urination;
- pale skin of the arms and legs (cyanosis);
- vomit.
Older children may complain of the following ailments:
- cough;
- nausea;
- abdominal or chest pain;
- swelling in the legs, feet, and face;
- shortness of breath or breathing problems at rest or at night;
- weight gain.
Danger and complications
Major complications include chronic heart failure (CHF), thromboembolism, heart valve defects and chronic inflammatory conditions.
- CHF is caused by a decrease in contractile and pumping function. It is based on myocardial damage and valve pathology.
- Thromboembolism is a serious complication of endocarditis. If a blood clot ruptures, depending on its location, it enters either the pulmonary circulation, leading to blockage of the pulmonary artery, or the large one, provoking an acute disturbance of blood flow in various internal organs: the spleen, brain, limbs, gastrointestinal tract or retina eyes.
- A protracted chronic process. Long-term persistence of microbial agents in the bloodstream can lead to the appearance of new purulent metastases in the body, as well as to the generalization of infection with the development of sepsis.
Along with cardiac complications, endocarditis can initiate renal and hepatic failure, embologenic infarction or stroke, inflammation of the meninges, intracranial abscesses, abscesses in the liver and lungs, thrombosis, angiitis, phlebitis, pneumonia and hepatitis.
Treatment of myocarditis
Since myocarditis is a disease that threatens serious complications, its therapy must be comprehensive. Much depends on the responsibility of the patient himself, since taking medications is not everything. It is very important to maintain bed rest, avoid physical activity, and maintain proper nutrition.
The diet for myocardial inflammation should be varied, rich in protein, unsaturated fatty acids, vitamins and microelements. Potassium and magnesium are especially important.
If inflammation has developed against the background of a chronic disease, such as an allergic or autoimmune reaction, appropriate therapy must be carried out - until the cause of myocarditis is eliminated, treatment will not be successful.
As for specific drugs, the following are prescribed:
- antibiotics – if the inflammatory process is caused by bacteria;
- antifungal, antiparasitic drugs - if the corresponding pathogen is identified;
- antiviral drugs - if myocarditis is of viral origin;
- non-steroidal anti-inflammatory drugs;
- salicylates;
- corticosteroids;
- immunomodulators;
- antihistamines.
These groups of medications help relieve inflammation and swelling. But in order for the heart to restore its function, this is not enough, therefore, in addition to the anti-inflammatory complex, drugs are prescribed that improve the activity of the heart:
- cardiac glycosides;
- coronary agents (dilate the heart vessels);
- antiarrhythmic drugs;
- drugs that improve metabolism in myocardial cells;
- vitamin complexes.
To speed up the healing process, physiotherapy is also indicated, in particular oxygen cocktails or inhalations.
After recovery, be sure to undergo sanatorium treatment. The patient is under clinical observation for a year.
Principles of treatment The main focus is on etiotropic therapy and treatment of complications.
Hospitalization is usually indicated. General measures include bed rest, oxygen inhalation, and nonsteroidal anti-inflammatory drugs (NSAIDs).
According to modern concepts, treatment of viral myocarditis should be based on the phase of the pathological process. According to the results of large international studies, the use of immunosuppressive therapy is justified in the presence of autoimmune disorders.
Etiotropic treatment of myocarditis
1. Viruses
Enteroviruses (Coxsackie viruses A and B, ECHO viruses, polio virus). The most common cause of infectious myocarditis. Treatment: maintenance therapy. Limit physical activity. Glucocorticosteroids (GCS) are not indicated. Recovery usually occurs within a few weeks, but ECG and EchoCG abnormalities may persist for several months.
Mumps, measles, rubella virus. Treatment: maintenance therapy. Immunization for the purpose of primary prevention.
Influenza viruses, A and B. Treatment: rimantadine, 100 mg orally 2 times a day for 7 days from the onset of symptoms.
Immunization for the purpose of primary prevention. Rimantadine is used for influenza A, treatment begins no later than 48 hours from the onset of symptoms.
Ribavirin is also active in vitro against influenza B viruses, but its effectiveness has not been proven (not approved by the FDA).
Dengue fever virus. The disease occurs with fever and rash and is transmitted by mosquitoes. Treatment: maintenance therapy.
Varicella zoster virus (chickenpox, shingles), herpes simplex virus, Epstein-Barr virus, cytomegalovirus. Treatment: acyclovir, 5-10 mg/kg, intravenous infusion every 8 hours.
Ganciclovir, 5 mg/kg, intravenous infusion every 12 hours. For myocarditis caused by the varicella_zoster virus and herpes simplex virus, acyclovir is prescribed, for cytomegalovirus infection - ganciclovir or foscarnet.
Considering the multifactorial etiology of the disease, therapeutic measures should be organized depending on the cause that caused the inflammatory process. The main method is drug therapy offered by official medicine. Home methods for improving the heart muscle are well complemented by medicinal effects.
Drug therapy includes the following areas:
- Fighting the pathogen.
When treating myocardial inflammation, drugs are prescribed that can kill or sharply weaken infectious agents. At the same time, complications such as arrhythmias and heart failure are treated (prevented).
Bed rest will be required for a period of one week to one and a half months.
A patient in a hospital is prescribed oxygen inhalation.
The diet limits table salt, liquids, and spicy foods.
For anti-inflammatory purposes the following is used:
- antibiotics;
- corticosteroids;
- non-steroidal drugs;
- salicylates.
For viral etiology:
- antiviral agents;
- immunomodulators to stimulate self-defense.
According to indications, you may need:
- cardiac glycosides;
- antiarrhythmic drugs;
- coronary agents to dilate coronary vessels;
- vitamins;
- agents that support metabolism in myocardial cells (Panangin, Mildronate).
For the treatment of autoimmune and allergic processes the following is used:
- antihistamines;
- large doses of corticosteroids;
- immunosuppressants that suppress excessive reactions.
For idiopathic myocarditis, cure is possible only by transplanting a donor's heart.
Like any other disease caused by bacteria, inflammatory heart diseases are mainly treated with antibiotics (and in the case where the inflammation is caused by viruses, with antiviral drugs).
Since the consequences of a disease not treated quickly and efficiently can be very serious, antibiotics are most often administered intramuscularly or even intravenously.
It goes without saying that treatment should be carried out only in a cardiology hospital, so that if necessary, doctors have the opportunity to immediately provide assistance to the patient.
In addition to antibiotics, medications are used to alleviate the patient’s condition. To remove excess fluid from tissues with the help of diuretics, to support the heart and nourish it so that it contracts more efficiently, to prevent the development of blood clots - all this is actively used.
If the treatment is carried out efficiently, inflammatory diseases will pass without leaving a trace and will not cause significant disturbances in the functioning of the heart. The main thing is to immediately consult a doctor at the first signs of illness.
Which doctor should I contact?
Any problems of the cardiovascular system, including endocarditis, are within the competence of cardiology doctors.
If such specialists are not available at your place of residence, you must come to an appointment with a therapist at the outpatient department, who will then issue a referral to a consultation with the appropriate doctor.
Follow-up care of patients is carried out by a cardiologist . The latter, after carrying out the required minimum of diagnostic measures, will choose an adequate treatment tactic.
Depending on the degree of damage to the patient’s heart, the curator can convene a consultation with the involvement of a bacteriologist, cardiac surgeon, ophthalmologist and other specialists to resolve the issue of either surgical intervention or continuation of conservative drug therapy.
Drug treatment
How to relieve inflammation of the heart muscle? To do this, the causes of the disease must be eliminated. Depending on the nature of the inflammation, the attending physician prescribes appropriate medications.
Drug treatment for myocarditis may include:
- Antimicrobials (antibiotics) to fight bacterial infection.
- Steroids to reduce swelling.
- Intravenous administration of immunoglobulin to increase the amount of antibodies necessary to combat the inflammatory process.
- Diuretics to remove excess water from the body. This reduces the load on the heart.
- Drugs to normalize heart rhythm. These include ACE (angiotensin-converting enzyme) inhibitors, beta blockers and angiotensin receptor blockers, which may be prescribed to treat pulmonary hypertension.
- Blood thinners to reduce the risk of blood clots.
- Drugs for the treatment of heart failure due to weakening of the heart muscles.
In rare cases, drugs may be used to suppress the body's immune response for autoimmune diseases.
Diagnostic algorithm
Physical examination:
- Anamnesis collection . Questioning the patient to identify previous infectious diseases, especially rheumatism, as well as the presence in the medical history of episodes of surgical interventions or therapeutic and diagnostic manipulations.
- Visual inspection . An indirect sign of endocarditis can be pustular rashes, skin symptom complex (petechiae, hemorrhages, Osler nodes, Roth spots), as well as the presence of rheumatic deformation of the joints. Impaired blood supply to tissues is detected by anemic skin, acrocyanosis of the tip of the nose, lips and fingers, as well as asthenic syndrome.
- Palpation . This method does not have an important diagnostic value, however, with sepsis, regional lymph nodes may enlarge: axillary, mental and inguinal. When palpated in the area of the cardiac impulse, its usual localization is often changed - in the fifth intercostal space.
- Percussion . This method of tapping the borders of the heart makes it possible to determine an increase in its size, which is often observed in endocarditis due to hypertrophy of the left ventricular myocardium and congestive heart failure.
- Auscultation . A fairly informative method that allows you to determine, using a stethoscope, the weakening of the first and second sounds in the area of the projection of the heart valves, as well as pathological noises.
Laboratory diagnostics:
- General blood analysis:
- normochromic anemia;
increase in ESR;
- shift of the leukocyte formula to the left;
- thrombocytopenia;
- dysproteinemia.
- Biochemical blood test:
- hyperalpha- and gammaglobulinemia;
high levels of circulating immune complexes, C-reactive protein and creatinine;
- increase in Ig M titer;
- detection of positive rheumatoid factor.
- Bacteriological analysis:
Identification of the pathogen plays the most important role in diagnosing the disease.
In the case of acute pathology, biological fluid is taken three times at 30-minute intervals, and in subacute cases - 3 times during the day. This number of samples eliminates the possibility of accidental insemination of the biomaterial with pathogenic microorganisms, which distorts the veracity of the results obtained.
Instrumental research methods:
- ECG . This method is not specific and only indicates the presence of a disturbance in the blood supply to the myocardium and arrhythmia (blockade), which can be observed in many cardiac pathologies.
- Echo-KG . It is the “gold standard” among non-invasive methods for diagnosing the disease, since it allows one to establish the presence of thrombotic vegetations on the leaflets of one’s own or prosthetic valves, so characteristic of endocarditis.
- X-ray . Determines the size and boundaries of the heart, congestion in the pulmonary circulation and other indirect signs of heart failure - a common complication of inflammation of the heart.
- Ultrasound, MRI and CT . Rarely used in everyday medical practice due to their high cost and technical complexity. However, they are indispensable in case of a complex clinical picture of the disease.
Differential diagnosis is carried out with such pathologies as:
- fever of unknown origin;
- septic conditions;
- some types of malignant tumors;
- infectious diseases that occur with febrile fever, skin rashes and enlarged spleen (salmonellosis, brucellosis);
- systemic necrotizing vasculitis;
- lupus erythematosus;
- rheumatoid polyarthritis with system-wide manifestations.
Diagnostics
When the myocardium becomes inflamed, it is impossible to do without a comprehensive examination. Questioning, history taking, and physical examination give the general picture, but the following tests are necessary to make an accurate diagnosis.
Electrocardiography is a fairly informative study. The cardiogram shows one or more of the following abnormalities:
- prolongation of electrical ventricular systole;
- bundle branch block;
- atrioventricular block;
- violation of intraventricular conduction;
- extrasystole;
- atrial fibrillation;
- sinus tachycardia;
- ectopic rhythms.
Blood culture
It is prescribed in any case to identify the causative agent of the disease. If the test results are negative, you should think about other causes of inflammation (viruses, parasites, allergens, etc.).
Detailed blood test
Allows you to determine the severity of the inflammatory process, the degree of disruption of the heart.
Radiography
It is carried out to assess the condition of the small blood circle and identify cardiomegaly (an increase in the size of the transverse size of the cardiac shadow) - these are clear signs of myocarditis.
Echocardiography
That is, ultrasound of the heart. An informative study that allows you to accurately assess the degree of damage to the heart muscle, the size of the inflammation, the condition of the valves, ventricles, and so on.
Endomyocardial biopsy
Prescribed to determine the causes of cardiac hypertrophy in any cardiomyopathy. An auxiliary method applicable in severe cases.
It is carried out to identify the inflammatory infiltrate in the heart muscle. The same applies to auxiliary methods.
Basically, ECG, echocardiography, blood culture, and complete blood count are used to diagnose myocarditis. Other types of research are carried out as necessary.
Diagnosing a disease when it is latent is quite difficult. Many patients consider the manifestation of weakness to be the norm after recently suffering from viral and infectious diseases and refuse to visit a doctor.
During the initial examination, the specialist asks the patient questions about the symptoms that appear.
A clinical blood test of a patient with suspected myocarditis reveals:
- increased number of leukocytes in the blood;
- an increase in ESR - erythrocyte sedimentation rate;
- increase in eosinophils.
Additional studies are:
- It should be remembered that bacteriological blood culture allows one to determine the causative agent of the disease.
- If you suspect an allergic nature, you should undergo an allergy test.
- X-ray examinations can reveal structural changes in the cavities of the heart and determine the presence of congestive processes in the lungs.
- Ultrasound examination helps confirm conduction disturbances and changes in heart rhythm.
- Only as a last resort do they resort to a heart biopsy.
Inflammation of the heart muscle always requires treatment.
serdce1.ru
Physical examination varies from moderate tachycardia to symptoms of decompensated right and left ventricular failure (swelling of the jugular veins, edema, weakening of the first tone, gallop rhythm, systolic murmur at the apex, congestion in the lungs).
X-ray of the chest sometimes reveals expansion of the borders of the heart and/or signs of pulmonary congestion.
ECG: usually there are transient nonspecific changes in the ST segment and T wave. Often in patients with acute myocarditis, pathological Q waves and a decrease in the amplitude of R waves in the right precordial leads (V1-V4) are recorded.
Since in the acute phase of myocarditis the activity of cardiac isoenzymes is usually increased, this, together with the indicated ECG changes, may lead to an erroneous diagnosis of myocardial infarction. Ventricular and supraventricular extrasystole are common, and atrioventricular conduction disturbances are less common.
Episodes of atrial fibrillation, as well as bundle branch block (usually the left one), indicating extensive myocardial damage, indicate an unfavorable prognosis.
EchoCG: depending on the severity of the process, varying degrees of myocardial dysfunction are detected (dilation of the heart cavities, decreased contractile function, often of a segmental nature, impaired diastolic function). In patients with subacute and chronic myocarditis, as well as in DCM, significant dilatation of the cavities of the heart is detected.
Intracavitary thrombi are a common finding.
Isotope study of the heart: with 67Ga, 99mTc_pyrophosphate and monoclonal antibodies to actomyosin labeled with 111In, magnetic resonance imaging, positron emission tomography allow visualization of areas of myocardial damage and necrosis.
Endomyocardial biopsy: It is currently believed that the diagnosis of myocarditis can only be confirmed by endomyocardial biopsy, which, however, gives many false-negative and questionable results. When evaluating biopsy results, the Dallas diagnostic criteria are usually used.
Myocarditis is considered definite in the presence of inflammatory cell infiltration (at least 3-5 lymphocytes in the field of view of the light microscope) and necrosis or damage to cardiomyocytes. Detection of cellular infiltration and unchanged cardiomyocytes corresponds to a questionable diagnosis.
Data from repeated myocardial biopsy allow us to assess the dynamics and outcome of the process and talk about ongoing, resolving or resolved myocarditis. The degree of severity of myocarditis can be judged by the number of interstitial inflammatory cells and their qualitative composition, as well as the prevalence and severity of destructive changes in cardiomyocytes, and the presence of necrotic cardiomyocytes.
Blood cultures: Using blood cultures and other biological fluids, the viral etiology of myocarditis can be confirmed, which is also indicated by a fourfold increase in the titer of antibodies to viruses during the recovery period compared to the acute period.
In the detection and identification of an infectious agent, a special place belongs to the most modern molecular biological method of the polymerase chain reaction.
A dynamic comprehensive study of immunological parameters is important.
Diagnostically identifying inflammation of the heart muscle is difficult when the disease is latent. Patients often find it common to develop weakness after an infection.
When examining and interviewing a patient, the doctor should specifically ask about the symptoms of myocarditis. The above manifestations of heart failure clearly indicate a connection with heart disease, and the acute nature emphasizes the role of infection or other factors.
A blood test reveals:
- leukocytosis;
- shift the formula to the left;
- increase in ESR;
- significant increase in eosinophils.
Among the biochemical tests you should pay attention to:
- excess of the norm of gammaglobulins, immunoglobulins;
- the presence of C-reactive protein, seromucoid;
- growth of sialic acids and fibrinogen.
Bacteriological blood culture helps identify the pathogen.
If an allergy is suspected, an antibody titer test is prescribed.
X-rays can reveal expansion of the cavities of the heart and congestion in the lungs.
Treatment
Conservative
Antibiotic therapy is prescribed in a hospital setting after accurate identification of the strain of the microorganism . Preference in the treatment of endocarditis is given to broad-spectrum antibiotics. For fungal infections, Amphotericin B and Flucytosine are prescribed for a long time.
To maintain the functioning of the heart muscle and eliminate symptoms such as shortness of breath, high blood pressure and tachycardia, edema, ACE inhibitors, beta-blockers, aldosterone receptor antagonists, diuretics, and cardiotonics are used.
Surgical
The need for surgical treatment arises in case of complications . Surgical intervention involves mechanical excision of the altered valve with implantation of an artificial one in its place with additional sanitation of the source of inflammation with broad-spectrum antibiotics.
Pathological areas can also be treated with low-frequency ultrasound.
Myocarditis: causes of inflammation, symptoms and therapy
The diagnosis of “myocarditis” is made when the patient experiences inflammation of the heart muscle due to multiple causes. They can be infections or toxins, allergic and autoimmune reactions of the body. Myocarditis can be both an independent pathology and a sign of certain diseases, such as rheumatism, developing in this case along with pericarditis or endocarditis.
The disease can be acute, often becoming chronic. Symptoms caused by myocarditis can be both obvious and hidden. Accordingly, the diagnosis of pathology is not complicated only if there are signs of acute dysfunction of the organ as a result of a viral infection, otherwise making a correct diagnosis is difficult.
Today, a common situation is when the pathology affects fairly young people - from 30 to 40 years old. Myocarditis causes impaired blood circulation, deterioration of pumping function, and heart rhythm. The consequences of the disease are very serious, in some cases death cannot be ruled out.
Why does the heart muscle become inflamed and how does the pathology manifest?
Let's consider the reasons under the influence of which pathology can develop, since there are a considerable number of them:
- Most often, the development of the disease is provoked by viral infections, especially Coxsackie viruses, as well as adenoviruses, cytomegaly, influenza viruses and parvovirus, rubella and chickenpox, as well as hepatitis C virus and others.
- Bacterial infections take second place. Usually, staphylococci, salmonella, mycoplasma and pneumococcus, and Haemophilus bacteria have a negative effect on the heart muscle.
- The influence of parasites cannot be ruled out. These can be worms and protozoa. The former include curved trichinella and nematodes, the latter include amoebas, toxoplasma and trypanosomes.
- Myocarditis often occurs against the background of autoimmune pathologies that provoke inflammatory processes in the heart.
- Taking certain pharmaceutical drugs may have a negative effect. Some antimicrobial drugs, non-steroidal anti-inflammatory drugs, diuretics, anti-seizure and anti-tuberculosis drugs may have a similar effect. And this is by no means a complete list of “problem” substances.
- The disease can develop if the body is exposed to certain toxins - arsenic or lead. The use of cocaine, which damages the heart muscle, has a similar effect.
As for symptoms, it depends on the degree of myocardial damage, the localization of inflammation, the rate of progression of the process and its severity. Regardless of the accompanying circumstances, a characteristic feature is a disruption of the heart rhythm and problems with the contractile function of the organ.
As for other signs, their appearance depends on the provoking factor:
- In case of viral or infectious-toxic pathology, the signs become obvious with clearly defined intoxication. This type of pathology is often preceded by a prodromal stage, in which the symptoms resemble flu, skin rashes, pain in joint and muscle tissues are not excluded.
- If the negative impact is caused by an allergic reaction or infection, the pathology manifests itself after the disease has been suffered.
- If an infectious-allergic form has occurred, inflammatory processes manifest themselves several weeks after an exacerbation of the chronic pathology has occurred.
- In the medicinal form, symptoms become apparent 12-48 hours after taking the drug.
There are a number of general signs characteristic of the formation of the disease in question:
- There is causeless weakness and severe fatigue.
- Shortness of breath develops, which increases with physical exertion. However, it is possible that it will appear in a calm state.
- Coughing attacks and a feeling of heaviness in the right hypochondrium may occur.
- With severe myocarditis, swelling of the lower extremities and decreased urine volume are observed.
- Pain occurs in the area of the heart muscle, which can be paroxysmal or aching. As a rule, they do not depend on the presence or absence of physical activity and bother the victim for a long time.
- There is an increase in heartbeat or interruptions in work; victims indicate a feeling of stopping, freezing of the heart.
- Typically, body temperature does not change, although it is possible that the readings may rise to a subfebrile level.
- Sweating may increase.
- Soreness appears in the joints.
- Blood pressure readings are usually below normal.
- There is a pallor of the skin and a bluish tint, which is especially noticeable when looking at the tip of the nose, fingers, and earlobes.
- The pulse is either slow or rapid.
- Enlarged neck veins indicate heart failure.
With this pathology, an increase in the size of the heart muscle is observed, so that even a small infiltration focus in the organ can provoke arrhythmia, leading to death. Despite the extensive list of symptoms, when the pathology develops, only one or a few of them may appear; in a third of victims, symptoms are completely absent.
Traditional treatment of pathology
Treatment of myocarditis should be aimed not only at combating the provoking causes, but also at maximizing the load on the organ and monitoring its functionality.
At the initial stage of development of the pathology, bed rest is required from 7 to 45 days; with the development of symptoms, it is necessary to strictly limit physical activity.
Pharmacological drugs are used that can reduce the manifestation of symptoms and negative consequences.
They use substances that stabilize the functionality of the heart, soften the signs of circulatory failure - diuretics, eliminating excess moisture from the body, which reduces the load on the heart muscle. At the same time, the attending cardiologist constantly selects the required drugs, the group and dosage of which depends on the individual characteristics of the course of the pathology:
- Antimicrobial and non-steroidal drugs, corticosteroids and salicylates are used as anti-inflammatory drugs.
- In the presence of a viral etiology, antiviral drugs and immunomodulators are prescribed to stimulate their own defense.
- In accordance with the indications, cardiac glycosides, coronary lytics, dilators of coronary vessels, drugs against arrhythmia and drugs to maintain metabolism in the myocardium, and vitamin complexes are used.
- In the case of allergic reactions and autoimmune processes, antihistamines, corticosteroids in increased dosages, and immunosuppressants are used to suppress excessive reactions.
Heart failure poses an increased risk of myocarditis. If the therapy used does not produce the expected effect, the disease can progress to the need for organ transplantation, which is associated with a fatal risk of rejection or infection. After a transplant, it is possible to return to normal life in rare cases; taking immunosuppressants becomes a mandatory and permanent condition of life.
In case of pathology, patients are recommended to adhere to a diet low in animal fats and sodium. It is advisable to completely avoid salt, replacing it with herbs or synthetic substitutes. Accordingly, it is necessary to give up fast food and restaurant dishes. Quitting smoking and drinking alcoholic beverages is also recommended. In some cases, weight correction is necessary, since excess body weight leads to increased stress on the heart muscle.
Traditional medicine: simple recipes
Folk remedies can be used as an additional method of therapy. There are complex recipes using herbal preparations and simpler methods that include the use of one component. Let's start with simpler recipes:
- Mountain arnica in the amount of one large spoon is brewed in 200 ml of boiling water and kept for 30 minutes, filtered. Take twice a day after meals, washing down the medicine with milk. A single serving is two small spoons of infusion.
- Add crushed leaves and strawberries in the amount of four large spoons to 0.5 liters of boiling water. The drink is infused for three hours. You should drink it instead of tea, adding a little granulated sugar or natural honey for taste. The duration of such treatment is 30 days.
- To prepare a tincture of lily of the valley, pour the flowers of the plant into a bottle and fill the container to the top with 90% alcohol. The product must be infused for seven days in the dark and cool, then filtered and taken three times a day. A single dose is 20 drops.
- You can use lily of the valley infusion. A large spoonful of flowers is brewed in 20 ml of boiling water, infused for 60 minutes and taken throughout the day at intervals of 120 minutes in the amount of two large spoons.
- If you experience heart pain, use spinach seeds. It is required to consume three grams of the product three times a day, half an hour before main meals. The seeds should be washed down with warm, purified liquid.
- A simple and affordable remedy is natural flower honey, which must be eaten several times throughout the day with fruit, cottage cheese or milk. A single serving is a small spoon. It should be borne in mind that honey should not be taken with hot drinks, since such a remedy will provoke increased work of the organ and increased sweating.
- You can prepare a nettle decoction. Brew five large spoons of the ingredient in half a liter of boiling water, simmer over low heat for five minutes, filter. The product should be taken up to four times throughout the day, the volume of each serving is 0.5 cups. Before drinking, you need to add a little natural honey to the drink.
Traditional treatment: complex recipes
Let's look at more complex recipes that are used to treat myocarditis. In this case, possible intolerance to certain components should be taken into account.
- You need to grind 5 grams of oak bark and pour 250 ml of boiling water over it, let it sit for 20 minutes, and filter. Add 300 ml of vodka, freshly squeezed juice from one lemon and 300 ml of birch sap to the infusion. The product should be taken three times a day, washed down with an infusion of thyme or mistletoe (50 ml). A single serving of the product is one large spoon.
- You need to mix 30 grams of motherwort with the same amount of valerian, add 20 grams of anise seeds and the same amount of yarrow. Pour a glass of boiling water over the collection in the amount of a large spoon and steam for another 15 minutes, leave for 15 minutes, filter. It is necessary to drink the infusion in the morning, afternoon and evening periods. The volume of each serving is 100 ml.
- It is recommended to mix eight parts of mint leaves with four parts of fennel seeds, add two parts of lily of the valley flowers, pour a glass of boiling water over a large spoon of the mixture and keep in a water bath for another 15 minutes. The product should boil. Then it is filtered and taken in the morning and evening hours, a single serving is half a glass.
- To obtain a tasty and healthy medicine, you need to grind 250 grams of lemons, first removing the seeds. 100 grams of figs, 250 grams of natural honey and 50 ml of high-quality vodka are added to the mixture. After mixing, store the product in the refrigerator, taking it after meals in the morning and evening. The quantity of one serving is a small spoon.
- You need to mix a large spoon of crushed hawthorn berries, the same amount of crushed rose hips, add rose hips in the amount of two large spoons. Pour the mixture with half a liter of boiling water and leave it in a thermos overnight. In the morning, the product is filtered and should be taken up to five times a day before meals. A single serving is 50 ml of drink.
It is necessary to use folk remedies only after consultation with a treating specialist.
fitoinfo.com
Special symptoms in children
In childhood, this pathology is very rare. Most often in children it develops in an acute infectious form and is characterized by the following symptoms:
- acute intoxication of the body, manifested by weakness, headache, joint pain;
- inflammatory process in the endocardium;
- Blood clots appear on the affected endocardium, which contribute to the development of thromboembolism.
The course of childhood endocarditis does not differ from the development process in adults, but the symptoms increase rapidly , in addition, the treatment of the pathology also does not differ much. The destructive process affects all internal organs, especially the urinary system. Any infectious disease is a risk factor that needs to be treated immediately.
Pulmonary regurgitation, causes, symptoms, treatment
Important! Pulmonary regurgitation occurs due to congenital pathology, infectious endocarditis.
If the patient ignores the symptoms, the condition becomes severe. In this case, shortness of breath and pancreatic failure occur.
The main symptoms include diastolic murmur in the left edge of the chest, compaction in the pancreas. In rare situations, insufficiency and pulmonary hypertension begin to develop sharply. As a result, regurgitation progresses.
In most cases, serious treatment is not required. Doctors prescribe medications to eliminate the pancreas, the causes of pulmonary hypertension. In severe cases, the patient undergoes comprehensive diagnostics and examination. As a result, a decision may be made about the need to insert a prosthetic valve into the pulmonary trunk. Our specialists will select the appropriate valve size on an individual basis.
Course of the disease in HIV-infected people
HIV-infected patients most often develop nonbacterial thrombotic endocarditis (arrowroot). It occurs in 3-5% of virus carriers and in almost all AIDS patients. Typically, this form of pathology develops asymptomatically and less commonly causes thromboembolism. Anticoagulants are used for treatment to prevent the formation of blood clots. Therapy is carried out aimed at eliminating damage to the valve apparatus.
In this case, the infectious type of the disease is manifested by debilitating febrile fever, the development of non-absorbable pulmonary infiltrates and multiple organ failure. With this form, symptomatic treatment is prescribed together with intravenous antibiotics.
Surgery
Patients with more severe cases of myocarditis may require surgery or other interventions.
The following types of treatment are distinguished:
- Ventricular assist devices. They are a pump used when the heart cannot pump enough blood. Some of them are located inside the body, while others have parts inside and outside.
- Pacemaker. Installed in patients with bradycardia (slow heartbeat) and heart failure.
- Intra-aortic balloon pump (IABP) is a machine that helps the heart pump blood throughout the body. It is used when the organ is unable to pump enough blood on its own. A special balloon is inserted through the femoral artery in the groin and threaded into the aorta. The balloon deflates and inflates, saturating the blood with oxygen and thereby reducing the load on the heart.
- ECMO (extracorporeal membrane oxygenation). In this case, the blood is forced through a special machine to increase the amount of oxygen, and then transfused back into the body.
- Heart transplantation. An organ transplant may be necessary in very severe cases when the disease cannot be cured with medication. The patient is transplanted with an artificial or donor heart. The disadvantage of this operation is the need for lifelong use of immunosuppressive drugs. This therapy is mandatory to eliminate the risk of organ rejection.
Forecasts and preventive measures
The prognosis of the disease is largely determined by its stage, timely contact with a specialist and the correct tactics of drug therapy.
Prevention of the disease includes:
- Careful monitoring of patients with prosthetic valves, heart defects, and previous endocarditis.
- For some types of surgery, endoscopic procedures, urological and gynecological diagnostic tests, a prophylactic course of antibiotics is recommended.
- Elimination of foci of hidden infection: caries, tonsillitis.
- Prevention of ARVI, influenza and sore throat.
Only competent and correct diagnosis and adequate therapy will help to cope with the disease radically and with minimal risk of developing life-threatening complications.
Source: oserdce.com
Inflammatory heart diseases
The basis of some diseases of the cardiovascular system is the inflammatory process. Sometimes the inflammation is of bacterial origin, that is, pathogenic bacteria multiply endocardium ) or on the outer linings of the heart (in the area of the pericardium ) These bacteria cause purulent inflammation of the corresponding parts of the heart - endocarditis and pericarditis . In such cases, the cardiologist prescribes antibacterial medications that suppress the growth of bacteria. Antibiotics are prescribed for a long time and in large doses.
Inflammatory processes in the heart muscle can be of a nature other than bacterial. Most often they are caused by disturbances in the functioning of the immune system, which occur as a result of diseases not directly related to the heart (sore throat, flu). These disorders provoke heart diseases such as rheumatism . myocarditis . some forms of endocarditis and others.
The heart muscle can also be affected by bacterial waste products (toxins) during inflammation of various organs. Toxins entering the blood . are delivered with it to the heart. This happens not only during inflammatory processes. The main harm from drinking alcohol, for example, is precisely that it causes severe damage to the heart muscle, and for some people only a small amount of alcohol is enough to drink. In diseases of the endocrine system, hormones have approximately the same effect on the heart . secreted by endocrine glands . The result of all these toxic effects on the heart muscle is myocardial dystrophy . which usually goes away some time after the source of the toxins is eliminated.
For all questions related to the diagnosis and treatment of cardiovascular diseases, you can contact our medical cardiologist.
We remind you that no article or website can make the correct diagnosis. Need to consult a doctor!
Materials
Inflammatory heart diseases
These diseases include endocarditis, myocarditis and pericarditis. As a matter of fact, these names only classify diseases according to the area affected: endocarditis is a lesion of the inner lining of the heart, called the endocardium, myocarditis affects the heart muscle - the myocardium, and pericarditis means diseases of the external tissues of the heart - the pericardium. All these diseases can be either independent or complications of other diseases. At the same time, the nature and course of inflammatory processes also varies, depending on the origin of the disease.
If we summarize the information known to medicine, we can classify the inflammatory processes of the endocardium, myocardium and pericardium as follows:
- Inflammatory processes of infectious origin - as a rule, infective endocarditis. This disease can lead to the formation of heart defects, kidney damage and is generally considered a serious disease that can quite often lead to death. Infectious endocarditis (in principle, inflammation can spread to the pericardium or other tissues) can be caused by various microorganisms - most often the coccal flora and mycobacterium tuberculosis.
- Inflammation of an immune nature - such inflammation is caused by the deposition of an antigen-antibody complex in the cardiac tissues. This reason is the most common for the occurrence of all types of inflammation. Most often, such inflammations occur in rheumatism, chronic diffuse connective tissue diseases and others.
- Inflammatory processes caused by injuries to heart tissue or tumor processes - such inflammations are completely classified as pericarditis.
- Reactive inflammation - such processes can occur as a result of myocardial infarction or after targeted radiation therapy for malignant tumors.
Inflammation of various tissues of the heart is accompanied by peculiar symptoms. Myocarditis is accompanied by symptoms indicating a lack of blood circulation - shortness of breath, palpitations, swelling). On an ECG, this condition is manifested by the appearance of an altered T wave. Pericarditis has two types - dry and exudative. Dry pericarditis is accompanied by dull, constant pain in the heart area. With exudative pericarditis, in addition to pain, shortness of breath at rest and signs of insufficient blood circulation may be observed.
Why does the heart muscle become inflamed?
There are quite a few reasons that contribute to the inflammatory process in myocardial cells. The most extensive group of factors predisposing to disease are infections. Once in the body, they have a detrimental effect on the condition of all organs, including the heart.
Infectious agents causing myocarditis:
- Viral - herpes, influenza, hepatitis, chicken pox, measles, mumps, rubella, cytomegalovirus, adenovirus, parvovirus, Coxsackie virus.
- Bacterial - streptococci, diphtheria bacilli, rickettsia, spirochetes, chlamydia, staphylococci, enterococci, pneumococci, mycoplasma, salmonella.
- Fungal – cause candidiasis, spergilosis, actinomycosis, coccidiomycosis.
- Parasitic - nematodes, roundworms, tapeworm, trichinella.
- Class of protozoa - amoebas, trypanosomes, toxoplasma, schistosomes.
Other causes of heart inflammation:
Allergy. This is the body's reaction to the influence of certain factors. A burn injury causes extensive necrotic processes, which promotes the absorption of toxic elements and destruction products into the blood. They, in turn, provoke the production of autoimmune particles that attack myocardial cells. Transplantation of organs or individual tissues can lead to the body’s rejection of a foreign element, which is manifested by an inflammatory reaction.
Pharmacological allergies develop after taking antibiotics, diuretics, anti-tuberculosis drugs, non-steroidal anti-inflammatory drugs, anticonvulsants and antimicrobial drugs. The introduction of a vaccine or serum, stings of wasps, bees and other insects are also possible causes of the development of myocarditis. A rare type of allergic reaction - eosinophilic inflammation of the heart muscle, occurs against the background of allergic skin diseases, bronchial asthma, or sudden cessation of adrenocorticotropic hormone.
Rheumatism. Rheumacarditis (acute rheumatic fever) occurs under the influence of an infectious pathogen (hemolytic streptococcus). In this case, an autoimmune reaction of the body develops: the immune system produces antibodies that attack the heart tissue. Myocarditis of rheumatic origin is separated into a separate group, since its etiology is determined by two factors at once: autoimmune and infectious.
Toxins. Penetrating into the body, they affect the heart along with other internal organs. Among the sources of toxic elements are the following: alcohol, uremia in renal failure, carbon monoxide, medications taken in high doses, the presence of arsenic, lead, cocaine, and excess thyroid hormones in the body.
Radiation. Ionizing radiation is used as a treatment for cancer. If the chest area is exposed to radiation (for a breast tumor, for example), the heart can also be affected by radioactive rays. Signs of inflamed heart muscle in this case may appear after a long period of time (even after 10 years).
Autoimmune diseases. These include, first of all, systemic lupus erythematosus, scleroderma, and rheumatoid arthritis. Autoimmune diseases are often accompanied by myositis (inflammation of muscle tissue of any location and etiology). Myocarditis is a type of such pathology. All these conditions are united by an abnormal reaction of the immune system, the antibodies of which mistake the cells of one’s own body for foreign elements and begin to fight them.
These factors influence the development of myocarditis in both adults and children. But small patients are at greater risk, because heat exchange reactions in this category (especially in newborns) are in the formative stage.
Electric shock. Causes serious damage to the heart muscle, including myocarditis. Possible fatalities.
The idiopathic form of the disease (name - Abramov-Fiedler myocarditis) is diagnosed when it is not possible to establish the exact cause of heart inflammation.
Distinctive features: rapid progression leading to significant stretching of the heart chambers, acute course with severe symptoms, serious condition of the patient. Prognosis: death from heart failure or an attack of arrhythmia.
Causes and symptoms of inflammatory heart diseases
Inflammatory heart diseases include myocarditis - inflammatory damage to the heart muscle - myocardium, endocarditis - inflammation of the inner lining of the heart - endocardium and pericarditis - inflammatory damage to the heart lining - pericardium. The causes and symptoms of inflammatory heart disease vary significantly depending on which heart muscle is affected.
Causes of inflammatory heart diseases
Myocarditis, endocarditis and pericarditis can be independent diseases, or they can be part of another disease, that is, a complication. Often with rheumatism, endocarditis and myocarditis develop, in this case the disease is called rheumatic carditis. One of the serious human conditions occurs when both inflammatory processes occur together in different parts of the heart, for example, myocarditis together with pericarditis. However, most often these diseases occur separately.
Inflammatory heart diseases, caused by infectious inflammation, mainly infective endocarditis, are extremely severe, often fatal, leading to heart disease and kidney damage - glomerulonephritis. The inflammatory process of infectious origin spreads to the pericardium from other organs. Most often, pericarditis is caused by coccal flora and develops mainly with pulmonary tuberculosis.
There is also a so-called immune form of inflammatory heart disease. An antibody is deposited in the myocardial, pericardial or endocardial tissue, which begins the development of the inflammatory process. Most often, these diseases develop with rheumatism.
Another cause of inflammatory heart disease is injury or the presence of a tumor in the body. In this case, pericarditis usually occurs.
Symptoms of inflammatory heart disease
When different parts of the heart are affected, different manifestations of the disease are observed.
Symptoms of endocarditis
With endocarditis, the valve leaflets are deformed and a heart defect is formed. The period of occurrence of the defect varies from six months to two years. With infective endocarditis, the picture of the disease looks brighter than with rheumatic endocarditis. The patient complains of chills, profuse sweating, and fever. In addition to the heart, the kidneys are affected, increased bleeding and decreased hemoglobin levels appear.
When the myocardium is damaged, the patient experiences shortness of breath, palpitations with slight exertion, and in severe forms of the disease, an enlargement of the heart, liver, and rhythm disturbances.
Symptoms of pericarditis
Manifestations of pericarditis are manifested in two forms of the disease: dry and effusion pericarditis. With dry pericarditis, the patient is constantly bothered by dull pain in the heart area. Exudative pleurisy is more severe; patients complain of constant shortness of breath at rest and heaviness in the heart area.
Pericarditis can have a chronic course. The patient's blood pressure rises, the liver enlarges, first swelling of the lower extremities appears, and then ascites.
Treatment of inflammatory heart diseases
In any case, a person who is suspected of one of these diagnoses is subject to emergency hospitalization. The diagnosis can only be made after a thorough examination and examination. In case of a mild course of the disease, the patient observes the ward regime, and in case of a severe course - strictly in bed.
Patients are prescribed a diet using a minimum amount of salt and liquid. Antibiotics and non-steroidal anti-inflammatory drugs are prescribed as medications. In severe cases, administration of corticosteroid hormones is necessary.
The duration of treatment depends on the severity of the disease and the success of drug therapy.
Source: heal-cardio.ru
How does pathology manifest itself?
Signs of myocarditis (especially of an infectious nature) do not always appear immediately. Up to 8 weeks after the illness, a person may not be aware of the pathological processes occurring in the heart muscle. Therefore, having recovered from a sore throat, flu, or acute respiratory infection, it would not be amiss to check this vital organ for the presence of inflammation.
At the initial stage of the disease, a person may complain of a constant loss of strength. As myocarditis progresses, inflammation of the heart muscle is indicated by symptoms:
- the skin takes on a white tint;
- cyanosis of the extremities and nasolabial triangle is noticeable;
- shortness of breath that occurs with slight physical exertion;
- legs swell;
- possible cough and pain in the right hypochondrium;
- rise in body temperature;
- there may be pain in the joints;
- attacks of night suffocation;
- migraines, dizziness;
- decreased blood pressure;
- pulsating veins of the cervical region;
- the rhythm of the heartbeat is disrupted;
- when listening, heart murmurs are detected;
- pain localized in the chest (heaviness, burning, squeezing, tingling);
- increased sweating.
For the severity of symptoms, the area of myocardial damage matters: focal or diffuse. In the second case, the disease is more severe.