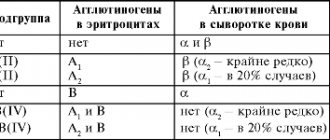
Diseases of the blood system are a very common phenomenon. Most often, the leukocyte unit is affected, but a condition occurs when the number of red blood cells in the blood, for various reasons, increases. This change is called erythrocytosis.
What it is, why it develops and what treatment is necessary for its development - the answers to these questions are in our article today.
Reasons for development
What are the main reasons for the increase in red blood cells in the blood of adults and children?
There are two main forms, the development of which depends on various reasons - true and relative erythrocytosis.
True erythrocytosis in children and adults is accompanied by an increase in the number of red blood cells against the background of various conditions and diseases. The following reasons can lead to its development:
- Diseases of the lungs and stomach. Histologically, the tissues of these organs contain cells capable of producing erythropoietin. An increase in the number of red blood cells is observed in chronic gastritis, COPD, and some oncological processes. These diseases are somewhat more common in men.
- Accommodation in high mountain areas. In this situation, the increase in the number of red blood cells is due to a change in the concentration of oxygen in the inhaled air. As many people know, mountain air contains less oxygen than the air we constantly inhale. Because of this, the body increases the number of red blood cells, which can bind more oxygen.
- Congenital genetic diseases and oncology. In this case, an increase in red cells is observed as a result of a genetic malfunction in the structure of certain proteins, which leads to increased production of red blood cells. The most common is Vaquez disease, which develops mainly in men over 40 years of age and somewhat less frequently in children.
Relative (or symptomatic) erythrocytosis occurs when the number of red blood cells is not increased, but in relation to other cells or plasma volume it is higher than normal.
Such conditions include loss of plasma as a result of shock or blood loss, taking certain drugs, massive burns and some intoxications. All of the above reasons are acquired and usually, after elimination, lead to the patient’s recovery.
Erythrocytosis - causes
According to statistics, polycythemia is diagnosed in patients of both sexes of different ages. The causes of erythrocytosis in women depend on its form. The most common ones include the following:
1. The primary anomaly is always a consequence of a hematopoietic defect at the genetic level or congenital heart defects.
2. Secondary polycythemia is an acquired phenomenon and therefore has several causes:
- carbon monoxide poisoning from smoking;
- living high in the mountains provokes hypoxia, which leads to an increase in the production of red blood cells;
- chronic diseases of the respiratory and cardiovascular systems;
- kidney diseases;
- oncology of various etiologies;
- relative erythrocytosis may occur as a result of prolonged menstruation or uterine bleeding;
- a lack of vitamin B12 in the female body provokes an increase in red blood cells;
- acute infectious diseases accompanied by vomiting and diarrhea;
- hypertension;
- stressful situations;
- overweight.
Main signs of the disease
Its main manifestations can be divided into stages:
- In the initial stages of many diseases, erythrocytosis can only be detected through directed laboratory tests (examination of bone marrow puncture, which reveals an increase in the number of all blood cells).
- At the second stage of erythrocytosis, changes are observed such as the development of hepatosplenomegaly, thrombosis of internal organs, and an increase in the concentration of certain biochemical parameters in the blood. In men, diagnosing erythrocytosis at this stage is much more difficult (due to changes in the internal organs and, mainly, the liver).
- In the later stages, despite the development of pronounced erythrocytosis, dysfunction of the liver and spleen is possible, the development of bleeding and subsequent anemia, the treatment of which poses significant difficulties.
These symptoms are accompanied by the development of headache, dizziness, thrombotic lesions of internal organs and spontaneous nosebleeds.
Symptoms of erythrocytosis
The norm of erythrocytes in adults ranges from 3.7 to 5.5 * 1012 g/l, starting with an indicator of 6, the level is considered elevated.
For more information about the normal values of red blood cells and the reasons for their deviation in blood tests in men and women, read the following links:
- for women
- for men
Signs of erythrocytosis depend on the stage of the pathological process, and may not be noticeable to a person at all until a clinical blood test is performed. The longer the underlying disease progresses or blood formation is impaired, the more often the patient experiences the following symptoms:
- dizziness (even to the point of fainting), painful headaches and migraines;
- heart pain (angina);
- brittle bones, fatigue, drowsiness due to increased blood viscosity and lack of oxygen in organs and tissues;
- deterioration of vision and hearing;
- unstable mood, excessive sentimentality and tearfulness;
- nosebleeds;
- bright red skin (especially on the face), difficulty in blood flow;
A person may suspect something is wrong, but only a doctor can confirm the presence of erythrocytosis based on the results of blood tests. Usually, in patients with erythrocytosis, with skin damage, the blood is viscous and thick, flows poorly, this is especially noticeable when taking a test.
Primary and secondary forms
As mentioned above, erythrocytosis can be divided into true and relative (depending on the reasons that caused it). However, there is another classification of erythrocytosis, according to which it can be divided into primary and secondary.
- Primary erythrocytosis develops against the background of a normal state of the body and the absence of a possible provocateur of the disease. This form of pathology is observed mainly in children. The main reasons leading to its development are violations of the genetic makeup of tissues and juvenile oncological diseases.
- Secondary erythrocytosis is a consequence of some pathological process. It manifests itself mainly in adults with one or more chronic or disabling diseases. It usually appears in men who abuse smoking.
Treatment of erythrocytosis
Therapy for symptomatic forms of the disease comes down to eliminating the cause that contributed to the increase in red blood cells, and for true polycythemia - chemotherapy.
If a violation of the ratio of plasma and formed blood particles is caused by tumor processes, they resort to surgery. Quitting smoking and normalizing body weight improve the prognosis. To improve the patient’s quality of life, symptomatic therapy is carried out and a diet is prescribed.
Drug therapy
The basis of treatment is drugs. To reduce blood clotting and the manifestations of the disease, the following drugs from different medicinal groups are used:
- Anticoagulants and antiplatelet agents – Trental, Heparin, Warfarin. To reduce the amount of thrombin, prevent atherosclerotic complications and blood thinning.
- Antihistamines - Suprastin, Loratadine. Used for symptomatic treatment. Eliminates skin itching.
- Preparations with acetylsalicylic acid - Aspirin, Methindol, TromboPol. Relieves headaches and prevents the development of thrombosis.
- Hypouremic agent – Allopurinol. Prescribed to patients with clinical manifestations of gout or urolithiasis. The drug removes excess uric acid from the body.
- General strengthening drugs – Interferon. Used to increase the body's resistance and prevent the development of vascular complications.
Medical nutrition
To reduce the number of red blood cells and hemoglobin in the blood, avoid foods with unsaturated fatty acids and vitamins K. Eliminate the following foods from the menu:
- fatty meat and fish;
- spinach;
- lettuce leaves;
- legumes;
- buckwheat porridge;
- coffee;
- strawberry;
- Bell pepper;
- carrot;
- pineapples;
- bananas;
- cabbage;
- kiwi.
Consume other fresh vegetables and protein foods in limited quantities. Do not forget about the drinking regime: the recommended volume of water per day is 1.5-2 liters. Add the following foods to your diet:
- ginger;
- lemon;
- grapefruit;
- egg white;
- unrefined vegetable oils;
- seafood;
- skinless chicken, turkey;
- garlic;
- greens (excluding spinach and lettuce);
- dairy products;
- nuts.
Physiotherapy
To enhance the therapeutic effect of medications, physiotherapeutic procedures are used. They are selected depending on the cause of erythrocytosis:
- For pulmonary diseases, heart pathologies, poisoning with toxic substances or carbon monoxide, oxygen therapy is prescribed. It helps prevent hypoxia, removes toxins from the body, and restores the functioning of the nervous system.
- If the increased level of red blood cells is associated with excessive activity of the bone marrow, bloodletting is resorted to. About 200 ml of blood is taken from the patient and the same amount of plasma replacement solution with glucose and anticoagulants is infused.
- Instead of bloodletting, hirudotherapy (treatment with leeches) or erythrocytepheresis (blood purification through a special device) is used. The techniques help avoid the formation of blood clots and improve blood circulation.
Traditional treatment
Additionally, decoctions and tinctures of medicinal herbs are used. Before starting treatment, consult your doctor. The following recipes help reduce blood viscosity:
- Pour 1 tbsp. l. green tea 500 ml boiling water. Add 1 tsp. grated ginger root, 2 lemon slices, 2 pcs. cloves, 1 tbsp. l. honey Infuse the drink for 15 minutes. Take tea every morning for 3-4 months.
- Pour 1 tbsp. l. dried sweet clover 600 ml boiling water. Leave for 2 hours. Take 100-150 ml before meals. The course of treatment is 3-4 weeks.
Erythrocytosis is an increase in the number of red blood cells (6 T/l or 6-1012/l and more) and hemoglobin (10.55 mmol/l or 170 g/l and above) in the blood.
Classification . Depending on the mechanism of occurrence, erythrocytosis is divided into absolute, caused by increased erythropoiesis in the bone marrow, and relative erythrocytosis , in which an increase in the number of red blood cells per unit volume of blood is a consequence of a decrease in plasma volume. According to etiology, acquired and hereditary erythrocytosis are distinguished.
Etiology . Acquired absolute erythrocytosis occurs with an increase in the production of erythropoietin 2 mainly in the kidneys under the influence of the following reasons:
1. violation of neurohumoral regulation - with stimulation of the sympathetic nervous system, hyperfunction of a number of endocrine glands 3 , which is often observed with tumors;
2. hypoxic, respiratory, circulatory hypoxia - for altitude sickness, chronic diseases of the lungs and circulatory system;
3. local hypoxia of the kidneys during their ischemia (hydronephrosis, stenosis of the renal arteries);
4. overproduction of erythropoietin by some tumors (hypernephroma, liver cancer, uterine fibroids, cerebellar hemangioblastoma, etc.). In addition, absolute erythrocytosis develops with a tumor of myeloid tissue - erythremia (polycythemia vera or Vaquez disease), which is a type of chronic leukemia.
The cause of hereditary absolute erythrocytosis may be a genetically determined increase in the formation of erythropoietin. With a hereditary deficiency of 2,3-diphosphoglycerate in erythrocytes (a regulator of oxygenation and deoxygenation of hemoglobin), the affinity of hemoglobin for oxygen increases and its release to tissues decreases (the dissociation curve of oxyhemoglobin is shifted to the left). Tissue hypoxia develops, the production of erythropoietin is stimulated, under the influence of which erythropoiesis increases.
Relative erythrocytosis occurs under the influence of the same causative factors that cause dehydration of the body (for example, increased sweating during hyperthermia, prolonged vomiting during intestinal obstruction and pyloric stenosis, diarrhea) or redistribution of blood leading to polycythemic hypovolemia (with shock, burn).
Pathogenesis . With absolute erythrocytosis, increased formation of erythropoietin leads to increased erythropoiesis with a subsequent increase in the content of red blood cells, hemoglobin, and hematocrit in the blood. In this case, polycythemic hyper- or normovolemia is observed, blood viscosity increases, and the function of the cardiovascular system is disrupted. Blood pressure rises, congestion of the internal organs, hyperemia of the skin and mucous membranes is noted, thrombus formation increases, and sometimes disseminated intravascular coagulation syndrome occurs (see p. 393 ).
Changes in the blood with acquired absolute erythrocytosis are often compensatory in nature and help improve oxygen supply to tissues under hypoxic conditions. With the cessation of the action of the etiological factor, the number of red blood cells and hemoglobin normalizes. However, with erythremia, erythrocytosis, which arises as a result of tumor proliferation of erythrocyte cells, does not have a compensatory value.
ANEMIA
Anemia is a hematological syndrome or an independent disease characterized by a decrease in the number of red blood cells and hemoglobin (or hemoglobin only) per unit volume of blood and changes in the qualitative composition of red blood cells.
CLASSIFICATION OF ANEMIA:
| by etiology: | hereditary, acquired; |
| by pathogenesis: | anemia due to blood loss (posthemorrhagic); anemia due to increased blood destruction (hemolytic), anemia due to impaired erythropoiesis; |
| by type of hematopoiesis: | anemia with erythroblastic type of hematopoiesis; anemia with megaloblastic type of hematopoiesis; |
| according to the ability of bone marrow to regenerate: | regenerative, hyperregenerative, hyporegenerative, aregenerative; |
| by color indicator: | normochromic (CP=0.85-1.15), hypochromic (CP<0.85), hyperchromic (CP>1.15); |
| by red blood cell size: | normocytic (average diameter 7.2 µm), microcytic (<6.5 µm), macrocytic (>8 µm); |
| according to the clinical course: | acute, chronic. |
The etiology of anemia is discussed in the relevant subsections.
The pathogenesis of anemia, along with the actual pathological disorders of erythron 4 , includes protective and compensatory reactions of the body. The first include changes in erythropoiesis, erythrodieresis, quantitative and qualitative composition of erythrocytes and hemoglobin, leading to the development of hypoxic syndrome (hemic type), associated with a violation of the main function of erythrocytes - oxygen transport. Compensatory reactions in anemia are aimed at eliminating or weakening hypoxia and are manifested by increased erythropoiesis (the leukoerythroid ratio in the bone marrow shifts from 3: 1 to 1: 1 and even 1: 3, in the blood the number of physiological erythrocyte regeneration cells increases), a shift in the oxyhemoglobin dissociation curve, changes in the functions of the circulatory and respiratory systems, tissue metabolism.
Symptoms of the disease Erythremia (polycythemia vera, erythrocytosis, Vaquez disease)
In the early stages of the disease, there are usually no symptoms. However, as changes in the blood supply system increase, patients complain of a vague feeling of fullness in the head, headaches, and dizziness. Other symptoms appear depending on which body systems are affected. Paradoxically, hemorrhage can be a complication of erythremia.
The advanced stage is characterized by more pronounced clinical symptoms. The most common and characteristic symptom is headaches, sometimes in the nature of painful migraines with blurred vision.
Many patients complain of pain in the heart, sometimes like angina pectoris, pain in the bones, in the epigastric region, weight loss, blurred vision and hearing, unstable mood, and tearfulness. A common symptom of erythremia is skin itching. There may be paroxysmal pain in the tips of the fingers and toes. The pain is accompanied by redness of the skin.
Upon examination, attention is drawn to the special red-cyanotic color of the skin with a predominance of dark cherry tone. Redness of the mucous membranes (conjunctiva, tongue, soft palate) is also noted. Due to frequent thrombosis of the extremities, darkening of the skin of the legs and sometimes trophic ulcers are observed. Many patients complain of bleeding gums, bleeding after tooth extraction, and bruises on the skin. In 80% of patients, there is an enlargement of the spleen: in the advanced stage it is moderately enlarged, in the terminal stage severe splenomegaly is often observed. Usually the liver is enlarged. Often in patients with erythremia, increased blood pressure is detected. As a result of malnutrition of the mucous membrane and vascular thrombosis, ulcers of the duodenum and stomach can occur. Vascular thrombosis plays an important role in the clinical picture of the disease. Thrombosis of the cerebral and coronary arteries, as well as the vessels of the lower extremities, is usually observed. Along with thrombosis, patients with erythremia are prone to the development of hemorrhages.
In the terminal stage, the clinical picture is determined by the outcome of the disease - liver cirrhosis, coronary thrombosis, a softening focus in the brain due to thrombosis of cerebral vessels and hemorrhages, myelofibrosis accompanied by anemia, chronic myeloid leukemia and acute leukemia.
The prognosis depends on the patient's age at diagnosis, treatment, and complications. Mortality is high in the absence of treatment and in cases where erythremia is combined with leukemia and other cancers.