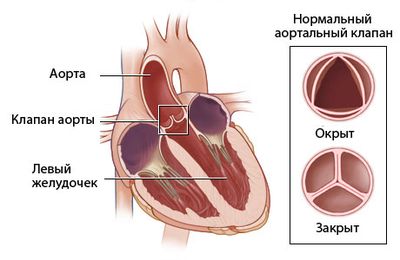
A violation of the structure of the aortic valve in medicine is called aortic defect (v. cordis aorticum).
The international classification of the ICD assigned this disease code Q23.
Aortic defects manifest themselves as follows:
- Aortic insufficiency is the incomplete closure of the aortic opening by the valve.
- Narrowing of the aortic valve.
- Aortic stenosis, coupled with aortic insufficiency, is a combined aortic defect characterized by stenosis of the aortic ostium and incomplete closure of the valve leaflets.
Aortic anomalies can be congenital; their clinical picture appears immediately after the birth of the child.
Acquired defects of the aortic system that arise during human life lead to hemodynamic disturbances in the body; the severity of the change depends on the degree of the disease.
Atherosclerotic defects
Aortic valve insufficiency
The anomaly is considered one of the most common problems in men and newborn boys.
The clinical picture is characterized by incomplete closure of the valve leaflet; through the remaining hole, part of the blood flow is thrown back into the left ventricle and overwhelms it.
The heart chamber quickly wears out, and blood begins to stagnate in the pulmonary arteries, which leads to pulmonary hypertension.
Aortic valve insufficiency can be congenital or develop rapidly immediately after the birth of a child.
The cause of the anomaly may be a genetic predisposition or an infectious disease of the mother suffered during pregnancy.
Aortic valve defects most often have a combined nature; isolated anomalies are less common.
Classification of the defect:
- valve leaflet atresia;
- depletion of valve tissue;
- hypertrophied valve;
- hole in the valve.
X-ray signs of the mitral configuration of the heart, description protocol.
The shape of the heart is of great importance in X-ray diagnostics. The most common heart diseases - valve defects, myocardial and pericardial lesions - lead to typical changes in the shape of the heart. Mitral, aortic and trapezoidal (triangular) shapes are distinguished
The mitral form is characterized by three signs (see Fig. 146): 1) the second and third arches of the left contour of the cardiovascular shadow lengthen and become more convex, corresponding to the trunk of the pulmonary artery and the appendage of the left atrium; 2) the angle between these arches decreases, that is, the left atriovasal angle There is no longer the usual normal retraction of the contour (“heart waist”); 3) the right atriovasal angle shifts upward. Let us add that often in diseases accompanied by a mitral heart, the left ventricle is enlarged, and then the fourth arch of the left contour is elongated and its edge is visible to the left than normal
This syndrome is recognized by a radiograph in anterior projection. The most important signs are lengthening and bulging of the second and third arches of the left contour of the cardiovascular shadow and a higher than normal position of the right atriovasal angle
Once it is established that the patient’s heart has a mitral shape, it is necessary to determine the size of each of its chambers. Without determining the size of the heart chambers, intrasyndromal diagnosis is impossible
The mitral shape of the heart occurs as a result of pathological processes that can be divided into three groups: 1) all processes accompanied by overload of the right ventricle - they cause an elongation of the second arch of the left circuit (most often this is the “pulmonary heart”); 2) processes that cause overload of the left atrium and right ventricle - with them, the second and third arches of the left circuit bulge and lengthen; 3) processes that cause overload of the left ventricle, left atrium and right ventricle - with them, all arcs of the left circuit, with the exception of the upper one, are enlarged -aortic arch
It is advisable to describe the x-ray picture of the most important diseases that cause mitralization of the heart, so that you are left with not a fragmentary, but a complete picture of these lesions. Mitralization of the heart due to overload of the right ventricle occurs with diffuse lesions of the lungs (chronic bronchitis, chronic emphysema, fibrosing alveolitis) Due to increased pressure in the pulmonary circulation, the large branches and the main trunk of the pulmonary artery expand, respectively, the second arch of the left contour of the cardiovascular shadow lengthens and becomes more convex. With increased load, the right ventricle expands and pulsates deeper than usual. Therefore, the lower arch of the right contour shifts to the right, and the atriovasal angle -up In the left oblique projection, the enlargement of the arch of the right ventricle and its deep pulsatory movements are clearly visible. Changes in the heart caused by the process in the lungs have received the common name “pulmonary heart”, or “pulmonary-heart syndrome”
Overload of the right ventricle can occur with some congenital defects of the heart and blood vessels. Let us point out two of them: non-fusion of the duct of Batal and narrowing of the pulmonary artery. In the first case, part of the blood from the aorta flows through the open duct of Batal into the pulmonary artery, which expands, and arterial plethora is detected in the lungs With pulmonary artery stenosis, the right ventricle has to experience increased load. It increases, its contractions deepen. Blood under pressure is ejected into the main trunk of the pulmonary artery, which expands in the initial part. But the branches of the pulmonary artery in the lungs have a small caliber. This sign is a discrepancy between the expansion of the main trunk and the small one. filling of the remaining vessels of the lungs - very indicative. Decisive evidence of congenital defects is obtained using artificial contrasting of the cavities of the heart and blood vessels
Overload of the left atrium and right ventricle occurs with stenosis of the mitral orifice. Due to the difficult passage of blood into the left ventricle, the left atrium expands. In the direct projection, elongation and bulging of the third arch of the left contour of the cardiovascular shadow is noted. In the right oblique projection, bulging of the left atrium arch is determined posteriorly with displacement of the esophagus along arc of small radius (up to 5-6 cm) Overflow of blood in the left atrium leads to an increase in pressure in the system of pulmonary veins and capillaries. To protect the capillary bed of the lungs, a reflex spasm of the pulmonary arterioles and small arteries occurs, which, however, leads to overload of the right ventricle. Thus , with mitral stenosis, there are two barriers to blood flow: the first barrier at the level of the mitral orifice and the second at the level of the pulmonary arterioles. In cases where venous stasis predominates, there is dilation of the veins in the upper lobes of the lungs or in all parts of the lungs. If pulmonary hypertension predominates (with a pronounced “second barrier”), the images reveal a peculiar picture: the pulmonary artery and its large branches are dilated, but small vessels are narrowed, as if suddenly “broken off,” and the pulmonary pattern on the periphery of the pulmonary fields even seems depleted. Septal lines appear
Due to the enlargement of the right ventricle, the lower arc of the right contour of the heart shadow shifts to the right, and the right atriovasal angle is located higher than usual. The left ventricle, which receives less blood than normal, pumps the same reduced amount into the aorta, therefore both the left ventricle and the ascending aorta are small in size ; their arches on radiographs are not changed or reduced
With the long-term existence of mitral stenosis, lime salts are deposited in the fibrous ring and valve leaflets. Calcareous accumulations are clearly visible during fluoroscopy and on tomograms of the heart. This is an important sign of mitral stenosis. The presence of calcification of the valve should be known to the surgeon when discussing the issue of surgical intervention - commissurotomy
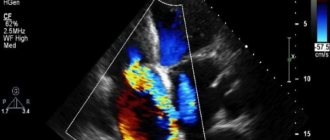
In recent years, ultrasound diagnostics (echocardiography) has gained leading importance in assessing the condition of valves and lime deposits in them.
27) Shapes and positions of heart shadow options.
The position of the heart in the chest cavity is determined by fluoroscopy, radiography in direct projection. The oblique position is characterized by an angle of inclination within 43-48°. The oblique position occurs mainly in people with a normosthenic build and is often combined with a normal heart shape. The vertical position of the heart is characterized by an angle of inclination ranging from 49 to 60°. It is usually combined with the mitral form and is characterized by the smallest transverse size and large long diameter of the heart. The horizontal position of the heart is determined by the angle of inclination within 3 0 ^ 2 °. The transverse dimension in a horizontal position is largest, the long dimension is reduced. The shape of the heart is aortic, the apex is raised above the diaphragm, the heart is widely adjacent to the diaphragm, the sharpness of the cardiophrenic angles is less pronounced. The horizontal position is found in hypersthenics (with obesity. The drop (hanging) heart occupies a special place among the extreme individual variants. The position of the heart is emphatically vertical, the angle of inclination approaches 60°, the shape is mitral as a result of bulging and lengthening of the arch of the pulmonary trunk. The size of the heart is small, Cardiodiaphragmatic angles are deep, emphatically acute. Drop heart is a constitutional feature of persons of extremely asthenic physique.
The shape of the heart is determined by fluoroscopy and radiography in direct projection. At the same time, the severity of the edge-forming arches of the cardiovascular bundle and the clarity of the delimitation of each of them, especially along the left contour, are analyzed. The usual shape of the heart is characterized by a smooth transition and smoothness of the arches of the pulmonary trunk and left atrial appendage along the left contour of the heart; it is not possible to draw a clear boundary between them. The arch of the aorta and left ventricle are most clearly visible. The true length of each arc of the cardiovascular shadow is determined by pulsation. As a variant of the norm, the usual heart shape is often found in people of normosthenic build. The usual shape of the heart is also observed in pathological conditions - diffuse damage to the myocardium (myocarditis, myocardial dystrophy), endocarditis, when the volumetric increase in individual cavities of the heart is not yet clearly expressed. The central shape of the heart is characterized by bulging and simultaneous lengthening of the arches of the pulmonary trunk and left atrial appendage or only one of them, namely the pulmonary trunk. The degree of bulging and elongation of these arches can be different - from barely noticeable to pronounced. The mitral shape of the heart is normally found in adolescents, in people of asthenic build, with a low position of the diaphragm. In this case, there is only a bulging of the arch of the pulmonary trunk without a volumetric increase in the right ventricle and expansion of the roots of the lungs. The mitral form is observed in diseases accompanied by the development of hypertension in the pulmonary circulation (mitral valve disease, cor pulmonale, patent ductus arteriosus, ventricular and atrial septal defect, etc.). The most typical mitral shape of the heart occurs with mitral defects, in which, as a rule, there is bulging and elongation of both arches - the pulmonary trunk and the left atrial appendage. In pathological processes, the formation of a mitral form is accompanied by a volumetric increase in the corresponding parts of the heart (left atrium, right ventricle, left ventricle), an increase in the angle of inclination, length and transverse size of the heart, a change (strengthening, sometimes depletion) of the vascular pattern of the lungs, expansion of the roots, as well as a violation myocardial functions. The aortic form of the heart is characterized by a projection shortening of the length of both middle arches along the left contour of the heart with the formation of their concavity. This creates a more emphasized rounding, 18 protrusion and elongation of the aortic arch and left ventricle. The heart is widely adjacent to the diaphragm, its apex is raised. The aortic form is found normally in children of the first year of life, in persons with a picnic build, especially when combined with increased fatness, and with a high position of the diaphragm (pregnancy, ascites). The pathological aortic form of the heart is observed in aortic disease, atherosclerotic cardiosclerosis, hypertension, coarctation of the aorta and other diseases. In this case, there is a volumetric increase in the left ventricle, changes in the shape, size and position of the aorta, dysfunction of the myocardium and vascular pulsation. The spherical shape of the heart is one of the variants of the normal shape, which is distinguished by a greater roundness of the right lower arch of the heart with the same smooth, without sharp boundaries, transition of both arches along the left contour of the cardiovascular shadow. The spherical shape is observed normally in early childhood and adolescence, sometimes in athletes, with moderate and uniform hypertrophy of the heart muscle of both ventricles. The spherical configuration reflects pathological changes in a number of congenital heart defects (ventricular septal defect, narrowing of the pulmonary artery, three-chambered heart, etc.), myogenic dilatation, effusion pericarditis. In this case, there are always signs of volumetric enlargement of the right ventricle with a violation of its contractile function and corresponding disturbances of blood flow in the lungs. The triangular shape of the heart is characterized by smoothness and straightening of the edge-forming arcs, their smooth transition into each other, a wide fit of the heart to the diaphragm, and the formation of straight or obtuse cardio-phrenic angles. A triangular heart shape is sometimes observed normally, particularly in children with a high position of the diaphragm (expiratory phase study). However, in the vast majority of cases it is a consequence of a volumetric increase in size, predominantly of the left ventricle. Therefore, with a triangular heart shape, a decrease in the tonic and contractile, and often conductive functions of the myocardium is usually noted, regardless of the etiology of the disease (myocarditis, atherosclerotic cardiosclerosis, secondary myogenic dilatation with heart defects, obesity, adhesive pericarditis, less often effusion pericarditis).
Symptoms of valvular aortic insufficiency
Usually, symptoms are not observed for several years, as compensatory mechanisms work.
An exception:
- acute heart failure;
- aneurysm;
- infectious endocarditis.
The clinical picture rapidly becomes more complicated, starting with the appearance of the following signs:
- high pressure;
- pulsations in the head;
- tachycardia;
- headache;
- dizziness;
- frequent fainting, especially when changing body position in space.
Further to these problems is added a symptom of right ventricular failure: swelling in the legs and difficulty walking.
In the absence of adequate treatment, death is likely.
Symptoms, signs, treatment
Often, aortic heart disease does not manifest itself for many years; when compression abilities deteriorate, it appears in the form of the following symptoms:
- Throbbing pain in the temporal part of the head and the back of the head.
- Noise in ears.
- Swelling of the legs.
- Pain in the chest area.
- Fatigue and fatigue.
- Dizziness.
- Heaviness on the right side of the ribs.
- Shortness of breath during light exertion.
During the diagnosis period, the doctor observes pale skin, abnormal blood pressure, tachycardia, enlarged heart, and cardiac hump. To confirm the diagnosis, ECG, echocardiography and phonocardiography are prescribed.
The first and second stages of the disease do not require special treatment from a cardiologist or therapist; it is enough to change the patient’s usual lifestyle and regularly undergo ultrasound examinations and ECG.
In the third and fourth stages of aortic insufficiency, drug treatment will be required, which consists of diuretics, cardiac glycosides, and beta-blockers.
Surgical intervention is prescribed for the congenital form of the disease upon reaching 30 years of age or after a sudden deterioration in the patient’s condition.
If the form of the disease is acquired, then surgical intervention will depend on the manifestation of pathological and physiological changes. A sharp deterioration in the functioning of the left ventricle or the critical condition of the patient may justify the operation.
Diagnostic measures
At the initial examination, the cardiologist notes pale, bluish skin, which in the later stages of the disease turns into acrocyanosis.
Patients often experience pulsating arteries, with the head moving in time with the beating.
Landolfi's syndrome can be observed - pulsations in the pupils, as well as Müller's syndrome (pulsations of the palate and uvula).
On palpation, the aortic pulse is felt in the seventh intercostal space, and a murmur is heard on the aorta, accompanied by Durosier's murmur.
Hardware diagnostics
Instrumental research methods include the following procedures:
- phonocardiography;
- radiography;
- MRI;
- Echo;
- catheterization;
- MSCT.
Main nuances of instrumental examination:
- An electrocardiogram is used to detect enlargement of the left ventricle and left atrium.
- A phonograph is needed to detect noise.
- Aortic insufficiency, changes in the valve structure and its anomalies are detected by Echo.
- Left ventricular hypertrophy, irregular apex of the heart, stagnation of venous blood in the arteries of the lungs are visible on x-ray.
- The quality of blood flow through the aortic valve is shown by aortography.
- To assess the degree of regurgitation, probing of the heart cavity is used.
Treatment of aortic insufficiency
There is no need to treat a mild defect; it does not require the introduction of special treatment measures; patients are recommended to reduce physical activity and have an annual examination by a cardiologist.
Medications for moderate aortic insufficiency:
- ACE inhibitors;
- diuretics;
- calcium blockers;
- drugs that block angiotensin receptors;
- antibiotics.
In severe cases, in the absence of effect from conservative therapy, surgical intervention is used. Patients undergo aortic and aortic valve replacement according to indications.
A poor postoperative prognosis is observed in people with an increase in the dialystic volume of the left ventricle to 300 ml, with a return fraction of more than fifty percent and a dialystic pressure of about 40 mmHg. Art.
This is an extremely difficult case; surgery is not recommended for patients with such problems.
How long do people with aortic insufficiency live? They can live up to ten years, depending on the degree of regurgitation.
Patients with acute coronary insufficiency die within two years after diagnosis.
Types and forms of aortic defects
Depending on the condition of the valve and the mouth of the aorta, several types of aortic heart defects are distinguished:
- insufficiency of the aortic valve (aortic insufficiency);
- aortic valve stenosis;
- combination of aortic stenosis with aortic valve insufficiency.
Aortic defects can be congenital or acquired. Congenital defects develop in the prenatal period and are detected by ultrasound diagnostics of the fetus. Such a defect can appear already in the first days of a child’s life and affect the functioning of not only the cardiovascular system, but also other organs.
To treat these diseases, medication or surgery is chosen. The treatment method depends on the severity and speed of development of the disease. The drug method helps relieve symptoms and stop further deformation of the valve and aortic mouth. Surgical treatment eliminates the cause and allows you to return to normal life without constant courses of medication after the rehabilitation period.
Narrowing of the aortic valve
This vice affects every second person who has crossed the sixty-year mark.
The narrowed mouth of the aorta and the destruction of its tissues lead to changes in the size of the heart and ultimately to heart failure.
Stenosis can be either congenital or acquired.
Picture of congenital stenosis:
- a growth of muscle tissue blocks the aortic valve;
- double-leaf or single-leaf valve;
- a hole is formed under the valve.
Congenital narrowing of the aortic orifice may not produce symptoms for several years, but as the child develops, clinical manifestations intensify.
Classification of the defect by severity:
- mild degree up to 1.6 sq. cm;
- average, 1 sq. cm;
- heavy - the clearance is already 1 sq.cm.
Clinical manifestations:
- pain in the chest, in the area of the heart;
- shortness of breath and feeling of heaviness;
- dizziness and fainting;
- swelling;
- chronic fatigue;
- nocturnal, cardiac cough;
At the initial examination, the cardiologist distinguishes patients with stenosis by the following characteristics:
- pale skin;
- weak and rare pulse;
- fainting state.
Auscultation confirms the diagnosis if the sound of the aortic valve closing is faintly heard, and during systole the noise of blood flow in the aortic valve is heard.
To clarify the diagnosis, cardiologists prescribe hardware examination methods:
- chest x-ray;
- ECG;
- Catheterization;
- Echocardiography through the esophagus and transthoracic;
- Dopplerography.
The defect is treated to a small extent conservatively, with drugs that normalize blood pressure and heart rhythm, as well as improve oxygen and cholesterol metabolism in tissues and blood.
Drug therapy:
- Antianginal agents: sustak; nitrong.
- Diuretics: furasemide; torasemide; britomar.
- Antibacterial: vancomecin; bicillin.
Antibiotics are prescribed before tooth resection or to treat tonsillitis, which can complicate the heart and cause endocarditis.
All recommendations for taking medications are provided by the attending physician.
If there is no effect from drug therapy, surgical treatment methods are used. Surgical repair of the aortic valves is used if the patient’s health is complicated by shortness of breath, constant weakness and other severe symptoms.
Surgical options for mitral-aortic valve stenosis:
- balloon aortic valvunoplasty;
- installation of an artificial valve.
The operation is contraindicated in patients over seventy years of age.
Symptoms
At first, aortic defects may be asymptomatic. The left ventricle is the most powerful part of the heart, so at first it can compensate for circulatory disorders. However, with the development of the disease, when blood is retained in it or returns to it more and more, it begins to stretch, its walls become thinner and can no longer cope with the load.
Because of this, organs and tissues lack oxygen and nutrients, and venous blood is retained in the vessels. These changes are responsible for the symptoms of aortic defects.
- A pressing or bursting pain appears in the area of the heart. This happens for two reasons. Firstly, a large amount of blood stretches the ventricle from the inside and puts strong pressure on its walls. Secondly, due to the fact that little blood enters the aorta, all vessels suffer, including those that feed the heart itself - the coronary vessels. Insufficient nutrition of the heart causes pain.
- Due to poor nutrition and lack of oxygen, the brain is primarily affected. This is manifested by weakness, dizziness, and sometimes fainting.
- Because blood is retained in the veins, the legs may swell.
- Shortness of breath occurs even during physical exercises that the person previously tolerated normally. As the disease progresses, it can appear even with a change in body position, and then at rest.
- To expel excess blood from the left ventricle, the heart begins to beat faster. This sign appears with aortic insufficiency. With stenosis of the aortic mouth, the opposite is true - the heartbeat slows down and the pulse becomes weak. Combined aortic disease is manifested by symptoms characteristic of the prevailing pathology.
- The patient may feel increased pulsation of blood vessels in the places where large arteries pass.
- These defects are characterized by rapid fatigue and decreased performance.
- A cough may appear at night.
Some signs also attract attention during an objective examination of the patient. Aortic valve defects manifest themselves with the following symptoms:
- Noticeable pallor of the skin,
- Tachycardia or bradycardia - depending on what kind of defect occurs,
- Large vessels pulsate strongly,
- There is a big difference between the upper and lower pressure,
- Excess blood in the heart puts a lot of pressure on its walls and peculiar turbulence occurs. When listening to the heart, this is manifested by a specific murmur,
- Since the valve flaps do not close completely, the sound of its closing is somewhat muffled.
Traditional methods of treatment
Traditional methods of treating atherosclerotic aortic valve disease include herbal medicine and the use of products that have a positive effect on blood vessels.
The composition of herbs and products that help restore the cardiovascular system includes beneficial substances - bioflavonoids.
Plant products in which bioflavonoids predominate:
- wine;
- grape;
- pine bark;
- nuts;
- rose hip;
- hawthorn;
- buckwheat flowers;
- red clover flowers;
- spiraea;
- nuts;
- sea kale.
The diet of patients with atherosclerosis includes honey with fresh onion juice, seaweed, garlic, blueberries, gooseberries, strawberries, currants, and chokeberries. Juices are useful, especially pineapple, beetroot and carrot.
To lower blood cholesterol levels, it is recommended to use hawthorn fruits containing nicotinic acid.
A decoction of hawthorn fruit is prepared as follows: pour one tablespoon of the raw material with a glass of boiling water and then simmer over low heat for fifteen minutes. You need to drink the product on an empty stomach.
Steroid glycosides necessary for normalizing heart function are contained in the plant Dioscorea nipponensis. The drug polysponin, used in therapeutic practice for the treatment of atherosclerosis, is obtained from its root.
For problems with blood vessels, it is recommended to use flaxseed oil, which has an anti-inflammatory and enveloping effect.
Pumpkin treatment
To clean the blood vessels, we take raw pumpkin, you need to start with twenty grams, once a day, gradually increase the dose to one hundred and fifty grams, three times a day. Pumpkin pulp is taken in a course of two months, then a week break.
Golden mustache tincture
Golden mustache contains the antioxidant quercetin. To prepare the tincture, take thirty joints of the plant and fill it with seventy percent alcohol (one and a half liter). We insist for two weeks.
For treatment, mix one teaspoon of tincture with one tablespoon of unrefined vegetable oil, drink it immediately, three doses per day.
The interval from taking the drug to meals should be at least two hours. The course of therapy with golden mustache tincture is ten days, then a break of five days.