Unfortunately, the number of patients with anemia increases every year. According to statistics, about 1/4 of the world's population suffers from anemia. In most cases, the disease occurs due to a deficiency of iron and other vitamins in the body. Much less often, the formation of the disease is associated with an imbalance in the volume of red blood cells in the blood. Anemia of the 1st degree - practically does not threaten the patient’s health. First-degree anemia can be treated wonderfully on an outpatient basis. In a fairly short period of time, specialists manage to completely and without any damage to the patient’s health, restore the function of blood formation
General information
Probably many people know what anemia is, since the disease occurs in almost every 6-7 inhabitants of the planet. Anemia is characterized by a sharp decrease in the concentration of hemoglobin and hematocrit in the blood (red blood rings). For men and women, all indicators are different.
For example, the norm of hemoglobin and hematocrit in the blood is:
- If in women the level is not lower than 120-125 g/liter. The hematocrit should be at least around 35-36%.
- If in men the indicators are not lower than 130-135 g/liter. The minimum hematocrit level is 39-40%.
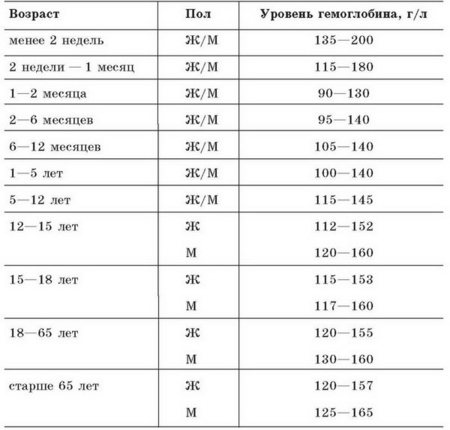
Table of hemoglobin norms in adults and children
Today, in almost 15-25% of the population, various types of anemia are diagnosed annually. As a rule, most cases of anemia occur in women, especially during pregnancy or lactation. Less commonly, you can find anemia that is associated with a deficiency of folic acid or vitamin B12, in other words, megaloblastic, aplastic anemia and, of course, the hemolytic form.
The most common is first-degree anemia, which develops against the background of iron deficiency in the blood (about 85-90% of all cases). Normochromic anemia occurs in about 30-35 of all cases. It should be noted that normochromic anemia can have a complex form (combinations of 2 or 3 types at the same time).
Causes of anemia
How to increase hemoglobin in a one-year-old child
Babies who are breastfed are less likely to show signs of anemia than those who are bottle-fed. This is due to the fact that human milk contains a special substance - lactoferrin, which increases the amount of absorbed iron. Infant formulas do not have such protein, so they contain more iron than the body requires in order to increase the percentage of absorption of an important microelement.
Red blood cells
The causes of anemia in an infant may be:
- refusal of a pregnant woman to take iron-containing medications;
- unbalanced nutrition of a nursing mother;
- bleeding;
- low percentage of food absorption (in infants, lactase deficiency leads to the development of anemia).
Important! If a child experiences increased abdominal bloating and diarrhea after each intake of breast milk or formula, you need to be tested for enzyme deficiency, and if detected, adjust the child’s diet, increasing the absorption of nutrients.
Varieties and stages
As a rule, in medical practice there are several main types of anemia:
- Anemia that occurs after significant blood loss.
- Diseases caused by a violation of the red blood cell ratio and their components (aplastic, megaloblastic, sideroblastic, iron deficiency anemia and those associated with chronic forms of diseases).
- Anemia, the formation of which is due to significant destruction of red blood cells.
Depending on the complexity and severity of the disease, three stages of anemia can be distinguished:
- Easy. If the hemoglobin level is in the range from 110-90 g/liter.
- Average. The amount of hemoglobin can fluctuate around 90-70 g/liter.
- Heavy. Hemoglobin in the blood is critically low (below 70-75 g/liter).
The content of red blood cells is normal and with anemia
Diagnosis of anemia
The diagnosis is established after a laboratory blood test, namely the number of red blood cells and hemoglobin.
They speak of anemia if the amount of hemoglobin is less than 110 g/l, red blood cells are less than 3.5 x 10¹²/l. These indicators correspond to a mild degree of anemia. Moderate anemia is established with the following indicators: hemoglobin less than 90 g/l, red blood cells up to 2.5x10¹²/l, severe anemia with hemoglobin less than 70 g/l, red blood cells less than 2.5x10¹²/l. When anemia is detected, the child is consulted by specialized specialists: gastroenterologist, nephrologist, allergist and others as appropriate.
Peculiarities
Almost every person who has even the slightest idea about the importance of blood in the body knows what grade 1 anemia means in an adult. This disease can be diagnosed in most patients, because the slightest deviations from the norm indicate the presence of grade 1 anemia.
There are a number of criteria by which type 1 anemia can be identified:
- The hemoglobin level is below normal by about 20% (in adults 95-115 g/liter of blood, in infants and children under 10 years old - 100-120 g/liter).
- A significant decrease in the concentration of iron in the blood serum (for men - 10-30 μ/mol, for women 10-20% less).
- A decrease in the number of red blood cells (for men 3.9-5.5 * 1012/l, for women - 3.5-4.5 * 1012/l, for children -2.5-3.0 * 1012/l.).
- The color index level is below 0.8-0.9.
Degrees of anemia
Depending on the reasons causing the development of anemia, morphological and pathological changes in blood cells, several groups of anemia are distinguished.
Posthemorrhagic
Anemia occurs due to rapid blood loss over a short period of time.
Severe bleeding can be caused by a traumatic factor or as a result of a surgical intervention, internal bleeding: peptic ulcer, lung diseases, etc.
Symptomatically, this type of anemia is manifested by palpitations, a sharp decrease in pressure (arterial and venous), and shortness of breath. On examination, pallor of the skin and mucous membranes is observed. The severity of symptoms is not directly proportional to the amount of blood lost. Some of them may be the body’s response to pain.
One of the significant signs of internal bleeding is the sudden, sharp appearance of a feeling of dryness in the mouth.
The severity of the condition is determined not only by the amount of blood lost, but also by the intensity of blood loss. The location of the bleeding matters: the accumulation of blood in the cavities is usually accompanied by severe pain (due to compression of organs), bleeding in the gastrointestinal tract may be accompanied by symptoms of intoxication, increased body temperature, etc.
A set of therapeutic measures for posthemorrhagic anemia begins with stopping bleeding.
Hemolytic
This form of anemia is a consequence of intense destruction of red blood cells. Therefore, laboratory confirmation of the diagnosis of “hemolytic anemia” is:
- With a hemogram: an increase in the level of free hemoglobin or bilirubin, which are products of the breakdown of red blood cells (erythrocytes). An increase in the number of reticulocytes (young red blood cells).
- A urine test reveals a dark yellow pigment: hemosiderin.
Main symptoms:
- jaundice;
- palpation determines the enlargement of the spleen;
- the formation of stones in the gall bladder can be caused by hemolytic anemia;
- modifications of the structure, shape and color (morphological changes) of red blood cells;
- percentage increase in reticulocytes in the blood (reticulocytosis).
Hemolytic anemias are usually hereditary conditions. With one of the varieties of hemolytic anemia - hereditary microspherocytosis - an additional characteristic symptom is the appearance of trophic ulcers in the lower leg area, which arise from an early age. Excessive formation of new cells by the bone marrow (hyperplasia) is the cause of impaired formation and formation of bones: malocclusion, high, prominent forehead, etc.
Hemolytic conditions include anemia caused by acute deficiency of glucose-6-phosphate dehydrogenase (G-6-PDG). In addition to the general clinical picture of hemolytic anemia, symptoms of G-6-FDG deficiency are pain in the bone tissue of the upper and lower extremities, elevated temperature, a sharp drop in blood pressure, up to the development of anemic coma.
Thalassemia also refers to fairly severe forms of hemolytic anemia. Bone marrow hyperplasia is strongly expressed: in addition to deformation of the bones of the head in the facial part, thickening and pathological development of the bone tissue of the cranial vault are determined by X-ray examination. Patients often suffer from infectious diseases. In a laboratory blood test, a characteristic sign is a change in the structure of red blood cells - they resemble a target, in the middle of which there is a spot of hemoglobin.
This is an incomplete list of hereditary conditions belonging to the group of hemolytic anemias. There are also hereditary stomacytosis, immune and autoimmune hemolytic anemia, paroxysmal nocturnal hemoglobinuria, and sickle cell anemia.
Aplastic (hypoplastic)
These are types of anemia in which the growth and maturation of 3 blood elements (leukocytes, erythrocytes and platelets) in the bone marrow progressively decrease, that is, hypoplasia develops (reduced formation of blood cells).
The main causes of the disease are toxic effects:
- chemicals;
- medicines.
The disease can be triggered by an increased dose of radiation, infectious microorganisms, and autoimmune processes. The reason for the high sensitivity of blood-forming cells to external influences is associated with their hereditary defects.
The etiology of idiopathic aplastic anemia (which does not develop due to the influence of any factors) remains unclear. The disease can develop gradually over a long period of time or begin in an acute form, with pronounced symptoms.
Clinical picture:
- A lack of blood cells (pancytopenia) provokes infectious complications and increased bleeding.
- A blood test reveals a reduced level of platelets and leukocytes, a low level of hemoglobin can reach critical levels (up to 20 g/l).
- In the bone marrow, areas filled with fat increase; areas of hematopoiesis are few in number, with low activity in the formation of new cells.
It is on the basis of histological analysis of the bone marrow that the diagnosis of aplastic anemia is finally made.
Dyserythropoietic
This group of anemias is associated with a decrease in the level of red blood cells: the replenishment of this blood element is insufficient due to its impaired division and the processes of destruction of red blood cells occurring in the bone marrow.
In the first type of dyserythropoietic anemia, megaloblasts can form in small quantities, the number of erythrokaryocyte nuclei is 2 or more. The disintegration of the cell nucleus (karyorrhexis) is a characteristic sign of the second type of anemia. Microcytosis (predominance of microcytes) and multinucleated (up to 12) erythrokaryocytes are symptoms of the third type of dyserythropic anemia.
The structure, shape, size and structure of erythroblasts remain within normal limits; morphological changes begin to appear in basophilic normoblasts.
Symptoms of the disease are similar to those of chronic hepatitis or jaundice (hemolytic type):
- yellowness of the skin;
- the size of the spleen and liver increases;
- Normal bone formation is disrupted: the skull is elongated, shaped like a tower, the little finger is shortened.
According to the results of the hemogram, pathological disorders of normoblasts are indicated by an increased level of unconjugated bilirubin.
Iron deficiency (hypochromic)
Anemia is associated with a low iron content in the body, which leads to impaired nutrition (trophism) of tissues. The altered function of respiratory tissue enzymes is manifested in dry skin, thin and brittle nails, and deterioration of the hairline.
In children, iron deficiency anemia develops in most cases due to insufficient intake of iron from the mother.
Symptoms
- Fatigue, chronic fatigue is accompanied by frequent headaches.
- Nails become brittle and hair falls out.
- Dyspeptic disorders, a sharp change in taste preferences (even perverted: patients eat chalk, earth).
- “Classic” signs of anemia: pallor, palpitations, and shortness of breath occurs with minor physical exertion.
The decisive test in making a diagnosis is a blood test confirming a low level of serum iron, hemoglobin, and color index.
Megaloblastic (B12-deficient and folate-deficient) are types of anemia, the distinctive features of which are a violation of DNA and RNA synthesis in cells (the appearance of megaloblasts).
Anemia due to vitamin B12 deficiency develops due to an insufficient amount of this substance entering the body or a violation of its absorption. Less commonly, B12 deficiency is caused by invasion of the broad lancet, which consumes reserves of this substance.
Children may develop Imerslund-Gresbeck syndrome, which affects the epithelium of the skin, intestines and kidneys; with this type of megaloblastic anemia, impaired absorption of vitamin B12 is accompanied by pathological damage to the kidneys.
The causes of idiopathic forms of megaloblastic anemia are not fully understood, although their genetic origin is often confirmed.
Clinical picture:
- the functions of blood formation, the functioning of the nervous and digestive systems are impaired;
- weakness that occurs with little exertion, palpitations;
- a burning sensation occurs on the tongue, its surface is polished (signs of glossitis);
- yellowness of the skin;
- the spleen (sometimes the liver) is enlarged.
The final diagnosis is made on the basis of a bone marrow examination: the level of elements of the erythroid series increases sharply with a predominance of enlarged cells - megaloblasts.
The folic deficiency state develops due to a lack of folic acid, which usually occurs as a result of its impaired absorption.
The clinical picture is identical to anemia caused by vitamin B12 deficiency. But with folic acid deficiency there are no signs of glossitis (polished tongue and discomfort in this area).
The diagnosis is made on the basis of a blood test: the amount of folic acid in red blood cells (in blood serum) is reduced.
Causes
There are many causes of anemia, due to which anemia occurs. They are different for each age group. In addition, the factors that contribute to the development of anemia differ by gender.
But it is still possible to identify some common causes of grade 1 anemia:
- Unbalanced diet (vegetarianism, various diets).
- Chronic diseases and inflammatory processes of the digestive system, which are accompanied by ulcerative neoplasms on the mucous membranes (ulcers, enterocolitis, etc.).
- Blood clotting disorder.
- Various injuries and injuries that are accompanied by extensive bleeding and lead to significant blood loss.
- Surgical interventions.
Among women
For women, it is worth adding a couple more causes of anemia:
- Frequent childbirth (once every 2 years). The female body simply does not have time to recover after significant blood loss.
- Early/late birth (before 18 years and after 30-35 years).
- Miscarriage of the fetus.
- Prolonged and severe bleeding with fibroids.
In pregnant women
During pregnancy, you need to carefully monitor your health. Anemia in a pregnant woman can lead to:
- A woman may even periodically lose consciousness.
- To the manifestation of early toxicosis.
- Low pressure.
- The placenta may detach from the walls of the uterus.
- To hypoxia (oxygen starvation) and other disorders during fetal formation.
- The risk of bleeding during/after childbirth increases.
- To premature birth.
In men
Causes of anemia in men:
- Excessive physical activity (sports training or military service).
- Prolonged and severe bleeding in diseases of the urinary system.
The child has
For children, especially infants, the cause of anemia may be:
- Prematurity.
- Impaired absorption of iron and other micro- and macroelements in the blood.
- Incorrect functioning of the circulatory system, or rather its defective formation.
- Worms (the impact on the child’s body of toxins that are released during the life of worms).
- Dietary disorders (early/late complementary feeding, unbalanced foods, etc.).
- Frequent viral infections.
- Impact of polluted environment on baby's health.
Why does anemia develop in children - all the reasons in the table
Table No. 1. Causes of anemia in children.
| Causes of anemia | Description |
| Antenatal (intrauterine) | The baby, while in the mother's womb, must receive the amount of iron necessary for normal development. Any pathological disorders during this period (late gestosis, threatened miscarriage, infectious diseases) lead to disruption of iron exchange between mother and child. Accordingly, an insufficient amount of iron accumulates in the child’s body for normal development. In addition, anemia can be passed on to a child “by inheritance” if a pregnant woman has this disease. This disease can be caused by too early childbirth and pregnancy with several babies at once. |
| Intrapartum (large blood loss during delivery) | The main reason for large blood loss is premature placental abruption, as well as too early or, conversely, late ligation of the umbilical cord. A woman can lose a large amount of blood if the umbilical cord is not treated properly, as well as if injured by obstetric instruments. |
| Postnatal | There are endogenous and exogenous postnatal causes of anemia. Endogenous anemia is a consequence of damage to red blood cells due to incompatibility between the blood of mother and baby (hemolytic disease of the newborn), as well as abnormalities in hemoglobin synthesis and the inability of the bone marrow to form blood cells. Exogenous anemia develops in babies under one year of age due to monotonous milk feeding. In addition, mother's milk may not contain enough iron, which is necessary for the development of the child. This type of anemia can be caused by early cessation of breastfeeding, poor-quality formula, and late introduction of complementary foods. |
Symptoms
Common signs and symptoms of anemia:
Poor appetite
- Feelings of weakness, fatigue. The person becomes more irritable. You may feel drowsy. As a result, performance is significantly reduced.
- Dizziness may occur. The patient is often bothered by headaches, sometimes there may be noise in the ears or flashing spots before the eyes.
- Increased heart rate even with minor exertion.
- Symptoms of shortness of breath appear at rest or with minor physical exertion.
Symptoms for different types of anemia may differ from each other. The symptoms of anemia are also influenced by the individual characteristics of the body. After all, each person is unique, and can react to a particular disease in different ways. The patient’s immune system also plays a significant role in creating resistance to the disease. Therefore, you should not diagnose yourself. If you have any health concerns, please consult a specialist.
In children with first degree anemia, pale skin may appear. The child begins to eat poorly. In addition, he is lethargic and no longer interested in games. A child with anemia can fall asleep independently during the day (not according to a routine). Nails are brittle and brittle. The baby may experience shortness of breath even with minor exertion. A child with anemia often begins to suffer from infectious and viral diseases. Older children may complain of severe headaches, dizziness, and rapid heartbeat.
Symptoms of anemia
Signs of anemia affect many organs and systems. The first visible signs appear on the skin, which becomes pale and flaky. Nails and hair become brittle, flake, and lose their shine. If you examine the earlobes in the light, you will see their transparency (Filatov’s symptom). The tongue may become inflamed, and aphthae (superficial ulcers) appear in the mouth. The nervous system suffers: babies become lethargic, whiny, they often feel dizzy, and there is noise in their ears. Sleep becomes shallow, bedwetting (enuresis), and fatigue may occur. Children who experience severe anemia before the age of 1 year may fall far behind their peers in development. Cardiovascular system disorders manifest themselves in low blood pressure, fainting, and rapid heartbeat. Systolic (at the moment of contraction) heart murmurs may appear.
Diagnosis and treatment
In order to identify anemia, the patient needs to undergo a number of examinations:
- Examination by a doctor.
- Complete blood count (for the number of red blood cells, reticulocytes, platelets and, of course, platelets; hemoglobin and hematocrit levels; MCV (mean erythrocyte volume), etc.).
Additionally, the specialist may prescribe other types of examinations in order to confirm or refute the diagnosis.
Treatment tactics for anemia (anemia) should be prescribed exclusively by a doctor, after your diagnosis is confirmed by tests and other examinations. For iron deficiency anemia, it is recommended to use drugs with a high iron content (Fenuls, Totema and others). It is advisable to use the medicine orally, since if the drug is administered subcutaneously or intravenously, there is a high risk of an allergic reaction. Additionally, it is recommended to consume ascorbic acid, which promotes the rapid absorption of iron.
Depending on the type and severity of anemia, different treatment regimens are prescribed, the results of which may appear in 2-3 months, or even later. In addition, after complete recovery, an additional preventive course of taking medications is carried out for 3 months (at lower doses).
If minor deviations from the norms are observed, do not panic! You can correct the level of hemoglobin in the blood not only with pills, but also with nutrition. In addition, walking in the fresh air will help you feel much better.
Treatment
Therapy for anemia is complex. In addition to general strengthening measures (sufficient physical activity, proper rest, time in the fresh air and a balanced diet), drug treatment and physiotherapeutic procedures are prescribed: gymnastics, massage, phototherapy with ultraviolet radiation.
Basic drug treatment:
- Iron supplements are prescribed (for example, hemofer, conferon, etc.).
- The duration of use of multivitamin complexes is at least 6 weeks.
In severe groups of the disease, surgical intervention is performed:
- Blood transfusion - blood transfusion (for example, with early anemia of prematurity).
- Complete or partial resection of the spleen (for hemolytic anemia).
- Bone marrow transplant (for aplastic anemia).
Dietary recommendations
Since in most cases of anemia occurs due to iron deficiency in the body, many experts recommend that patients consume more healthy foods high in iron. In addition, the patient's diet for anemia should be enriched with many other vitamins, since it has been proven that iron itself is not absorbed.
Iron-rich foods
Patients with anemia are advised to include the following foods in their daily diet:
- Egg yolk.
- Liver, beef heart, tongue dishes.
- Turkey meat.
- Dairy products.
- Nuts.
- Honey.
- Apples and peaches.
- Broccoli.
- Whole grain porridge.
- Dried fruits.
It is advisable to cook all dishes in a double boiler or eat them fresh!
Children under 6 months should not be given complementary foods! The baby receives iron and other vitamins from mother's milk or special infant formula. From 7-8 months, the child can be introduced to the diet with meat and fruit purees. Additionally, provide fresh fruit juices.
Expert opinions on the causes and treatment of anemia in children under one year of age and older
Candidate of Medical Sciences A. V. Malkoch:
Treatment of IDA (iron deficiency anemia) in young children should be comprehensive and based on four principles: normalization of the child’s regimen and nutrition; possible correction of the cause of iron deficiency; prescription of iron supplements; concomitant therapy.
The use of parenteral iron supplements is indicated to quickly achieve an effect in severe anemia... It must be remembered that in young children, iron deficiency is never isolated and is often combined with a deficiency of vitamins C, B12, B6, PP, A, E, folic acid, zinc , copper, etc. Therefore, it is necessary to include multivitamin preparations in the complex therapy of IDA.
The effectiveness of IDA therapy can be judged after 7–10 days by an increase in reticulocytes by 2 times compared to the initial number (the so-called reticulocyte crisis). If within 3–4 weeks there is no significant improvement in hemoglobin levels, then it is necessary to find out why the treatment turned out to be ineffective.
T.V. Shamanskaya, D.Yu. Kachanov, Federal State Institution Federal Scientific and Clinical Center for Pediatric Hematology, Oncology and Immunology of Roszdrav (Moscow):
Iron deficiency develops as a consequence of inadequate intake into the body, especially against the background of increased need or increased loss of iron in the blood. Risk factors:
- Accelerated body growth: premature babies, young children, teenagers.
- Insufficient intake of iron from food: - use of mixtures not fortified with iron; - use of whole cow's milk in children of the first year of life; - no additional administration of iron to children who are exclusively breastfed after 6 months of life; — diet disorders in adolescents; - vegetarianism.
- Loss of iron in the blood: - menorrhagia; - blood loss through the gastrointestinal tract; - Meckel's diverticulum; - esophagitis due to reflux disease - peptic ulcer; - inflammatory diseases of the large intestine; - parasitic infections; - idiopathic pulmonary hemosiderosis.
The goal of therapy for iron deficiency conditions is to eliminate iron deficiency and restore its reserves in the body. To do this, on the one hand, it is necessary to eliminate the causes that led to the development of IDA, and on the other, to compensate for iron deficiency in the body. It is impossible to compensate for iron deficiency in the body only by adjusting the diet, without taking iron-containing drugs.
Modern requirements for oral iron preparations used in pediatric practice include high bioavailability, safety, good organoleptic properties, the ability to choose the most convenient dosage form... These requirements are best met by preparations of iron (III)-hydroxide-polymaltose complex (Ferrum Lek , Maltofer).
A control blood test on the 7-10th day of therapy demonstrates an increase in the level of reticulocytes (reticulocyte crisis). Normalization of hemoglobin levels cannot serve as a basis for discontinuing iron supplements. Cure from IDA is indicated by overcoming tissue sideropenia, which is observed from 3 to 6 months from the start of therapy. Therefore, the only criterion for discontinuation of iron supplements is the normalization of serum ferritin levels.
What are the symptoms of initial anemia
Symptoms typical of first-degree anemia do not depend on the type of anemia and may not appear at all. The disease is detected unexpectedly during a routine examination. Most often the patient feels:
- weakness;
- increased fatigue;
- dizziness.
It is impossible to demand full dedication from an adult with grade 1 anemia in the workplace. WHO considers anemia to be the third leading cause of disability.
Some people, despite the mild degree of the disease, may experience fainting, palpitations with little physical activity, pale skin, and increased frequency of angina attacks.
Nutrition for anemia
Anemia rarely develops during breastfeeding, this is explained by the chemical composition and quality of absorption of mother's milk. Therefore, breastfeeding is one of the main preventive and therapeutic measures for anemia.
If this is not possible, then to ensure adequate nutrition, special mixtures are used, the composition of which was specially developed for children with anemia. Dry ready-made milk formulas (enpits) contain highly digestible, processed proteins and fats, enriched with B vitamins, folic acid, iron, etc. Due to the specific taste and color, medicinal enpits are mixed with breast milk or regular milk formulas. With age, they can be added to cereals, soups, and drinks.
The use of antianemic enpits is carried out under the supervision of a doctor: he prescribes the required dosage of the mixture, frequency and duration of administration.
The child should receive proteins, vitamins and microelements through complementary foods. The first supplements are fruit and vegetable juices and purees. In addition to their beneficial composition, they have a beneficial effect on the functioning of the gastrointestinal tract.
The schedule for introducing the first nutritional supplements for a healthy child is as follows:
- juices (usually carrot and apple) – from 5-6 months of age;
- grated vegetables and fruits - half a month later.
Complementary foods are introduced in small portions, with observation of the baby’s emotional and physical state: skin color (absence of allergic reactions), stool consistency.
For a child suffering from anemia, the first course of complementary feeding should be vegetable puree, since it contains the required amount of minerals. The first complementary foods are introduced earlier - from 4 months. First, it should be boiled vegetables, for example, boiled carrots or pumpkin mixed with an apple. From one year onwards, it is recommended to include salads made from raw vegetables and herbs in the diet. Porridge and meat (beef) puree are introduced from 6 months of age. It is better to give preference to buckwheat and oatmeal porridges rich in B vitamins, iron and microelements, brewing them in water, vegetable broths, breast milk, but in no case with cow’s milk.
From 7 months, fish, egg yolk and cottage cheese are introduced.
It is recommended to give lactic acid products to children with anemia no earlier than 1 year, limiting their intake to 1 glass per day.
Older children should definitely include liver and beef dishes, vegetables, fruits, greens in any form, seafood and legumes in their diet.
How to treat
The doctor prescribes treatment for anemia during pregnancy, taking into account the type and severity of the disease. Most often, vitamin complexes and iron supplements are prescribed. Also, a pregnant woman must follow a diet.
Vitamins
Vitamins are important for iron deficiency. To treat anemia use:
- Vitamin C. This is a natural antioxidant that allows the body to absorb ferrous iron. It is found in bell peppers, baked potatoes, citrus fruits, black currants, and cabbage.
- Vitamin E. Protects the placenta from the negative influence of internal and external factors. It is found in peas, spinach, parsley, green salad, tomatoes, rose hips, and vegetable oils.
- Vitamin B9. It is found in nuts, liver, yeast, and honey.
- Vitamin B6. Stimulates metabolism, helps to absorb protein from food, and is necessary for the synthesis of hemoglobin. Contained in meat products, nuts, fish, legumes.
- Vitamin B12. Due to its deficiency, anemia develops. It is found in yeast, milk, fish and meat.
In addition, treatment of anemia in pregnant women is carried out with special vitamin complexes. They contain all the necessary kit that is required to prevent complications.
Iron supplements
If anemia is diagnosed during pregnancy, treatment is carried out under the supervision of a doctor. The specialist prescribes medications containing iron. They help restore the necessary level of this microelement in the body. Such drugs are used in the form of tablets or administered intramuscularly, as well as using a dropper.
To cure anemia, the following effective medications are prescribed:
- Ferrocal - replenishes iron deficiency, which allows to enhance the formation of red blood cells in the bone marrow.
- Ferroplex - consists of iron and ascorbic acid. The latter promotes enhanced absorption of the microelement in the intestine.
- Conferon - the components included in its composition improve the absorption of iron in the intestines.
- Ferrum Lek is used intravenously and intramuscularly if it is not possible to take the microelement orally.
It is recommended to swallow capsules and tablets whole. The effect is observed after 3-4 weeks of taking the drug.
How can you tell if you have anemia?
It will be difficult for an ordinary person to diagnose first-degree anemia on his own. To identify this pathology, it is necessary to undergo several tests. You can go to the clinic to have them taken if you feel a constant loss of strength and get tired quickly during physical activity.
The diagnosis of mild anemia is made on the basis of data from a general blood test (CBC), biochemical blood test, and myelogram.
The following data is taken into account:
- The total amount of hemoglobin and its content in individual red blood cells;
- Color index (CI), which can be increased or decreased depending on the type of anemia;
- Changes in the size and shape of red blood cells;
- Serum iron level.
Even a mild degree of anemia can cause tachycardia, angina, and fainting. If you encounter these problems, consult your doctor to rule out more serious diseases.
Main reasons
Iron deficiency:
- Ferrum deficiency caused by chronic blood loss;
- Disorders in proteins that transport or store iron;
- Increased need for iron during pregnancy, lactation or intense physical activity;
- Deficiency associated with insufficient intake of this element from food.
Vitamin B12 deficiency:
- Insufficient intake of vitamin due to poor diet;
- Pathologies of substance absorption in the intestine;
- For gastritis;
- B12 deficiency as a result of helminthic infestation;
- For chronic liver and kidney diseases.
For aplastic type of pathology:
- Death of stem cells;
- Errors during bone marrow cell division;
- Due to hepatitis A;
- As a result of mononucleosis.
For hemolytic anemia:
- Tumors or autoimmune disorders in the body;
- Transfusion of blood components with incompatibility of blood groups;
- During pregnancy due to Rh conflict;
- As a result of the influence of poisons such as snake, bee, mercury or lead.
For posthemorrhagic anemia:
- Acute loss of a large amount of blood (and hemoglobin in its composition);
- The inability of the bone marrow to quickly replenish the normal volume of blood flow.
Anemia and pregnancy
Vitamin and mineral complexes will also not be superfluous, which will help maintain the condition of the mother and child’s organisms at the proper level.
Anemia of the 1st degree is a common occurrence among pregnant women. It appears as a result of an increased need for iron and other microelements.
The woman’s body is now obliged to supply the fetus with oxygen, so the bone marrow does not always cope with the increase in hemoglobin levels.
Its deficiency leads to oxygen starvation and the appearance of symptoms of anemia. This can be avoided by adding iron-rich foods to your diet.
Anemia in children
It is more difficult to detect anemia in a small child than in an adult. Children cannot objectively assess their own well-being, so parents should be vigilant.
A blood test is necessary if your child:
- Pale;
- Doesn't eat well;
- Gets tired quickly;
- Tries to eat meli and other unusual “food”;
- Has brittle nails or problems with hair loss;
- Complains of shortness of breath during physical exertion.
You can assess the condition of a baby by its skin tone and activity. If you notice any warning signs, get his blood tested. In children under one year of age, constant fluctuations in blood composition occur, so only a pediatrician can judge the presence of problems.
Anemia in infants is often caused by insufficient iron intake from mother's milk. If your child is diagnosed with this pathology, you should also take a blood test.
Approximate criteria by which one can judge the presence of anemia in a newborn child
| Full-term newborns | Premature newborns | |||
| Age | Hemoglobin level, g/l | Hematocrit number, % | Hemoglobin level, g/l | Hematocrit number, % |
| First hours of life | <180 | <40 | <160 | <45 |
| First week | <140 | <30 | <120 | <38 |
| Third week | <120 | <25 | <110 | <30 |
| First month | <115 | <25 | <100 | <25 |
The hematocrit number is the ratio of blood cells (mainly red blood cells) to its total volume. A drop in hematocrit and hemoglobin levels below these figures indicates that the child has anemia.
Classification and symptoms of the disease
Depending on the factors of occurrence and mechanisms of development of anemia in children, the classification is as follows.
Posthemorrhagic anemia
This type is caused by blood loss.
Acute posthemorrhagic disease is characterized by injuries caused by surgery, rupture of blood vessels, damage to the lungs, digestive tract, and cardiac cavities.
The symptoms are:
- pale skin;
- rapid pulse, tachycardia;
- temperature drop;
- fainting;
- severe dizziness;
- nausea and vomiting;
- the appearance of perspiration.
The symptoms are quite common, so a careful differential diagnosis is required.
Chronic type
Frequent minor bleeding of internal organs is characteristic. They are provoked by chronic diseases of the abdominal organs (gastroduodenitis, duodenal ulcer, biliary dyskinesia), kidneys, lungs, nosebleeds and other pathological disorders.
Symptoms of chronic posthemorrhagic disease are:
- increased body temperature (up to 37 degrees);
- symptoms of body poisoning;
- pain in the area of certain internal organs;
- decreased physical activity;
- sweating;
- swelling;
- dry mouth;
- parosmia (smell disorder).
A characteristic diagnostic criterion is the presence of acute or chronic bleeding before the onset of these symptoms.
Iron deficiency anemia in children (hypochromic)
Occurs due to a decrease in the level of iron in the body. Provoking factors are insufficient intake of iron-containing products, poor absorption of iron, and pathological losses.
The main factors causing the painful condition include:
- immature hematopoietic system;
- poor nutrition;
- helminthiases;
- infectious, tumor diseases;
- surgical interventions;
- hormonal imbalance in adolescence.
Iron deficiency anemia in children under one year of age often occurs due to a lack of iron intake from mother's milk, the use of unadapted formulas, violation of the introduction of complementary foods, premature birth, and during the mother's multiple pregnancy. There is a lag in physical and mental development.
Iron deficiency anemia has 2 stages of development: latent and the stage of clinical manifestations.
Before the first symptoms of the disease appear, it is in a latent (hidden) stage. There is a gradual decrease in serum iron, which does not affect health in any way.
The period of clinical manifestations begins after the iron reserves in the body are completely depleted.
Iron deficiency in children quite often manifests itself as pale skin and mucous membranes, poor appetite, cravings for non-food components, dental problems, poor sleep, and moodiness.
B12 folate deficiency (megaloblastic) anemia
The disease develops due to the lack or absence in the body of vitamin B12 (cyanocobalamin) and folic acid, which are involved in the formation of red blood cells in the bone marrow and the synthesis of the myelin sheath that covers the axons of many neurons. Due to the deficiency of these substances, the tissues of the nervous system and bone marrow are especially affected. The main factor in the development of this disease is the refusal of animal products (vegetarianism).
Deficiency of cyanocobalamin and folic acid is also provoked by:
- changes in normal intestinal microflora;
- low absorption by the body;
- dysfunction of the digestive system;
- helminthiases;
- increase in their needs (during periods of rapid growth);
- abnormal utilization.
Symptoms of B12-folate deficiency anemia include a number of signs.
Namely:
- weakness, decreased activity;
- pale skin;
- change in tongue color;
- sensitivity disorder;
- weight loss;
- decreased gastric secretion;
- malfunctions of the nervous system.
Hypoplastic and aplastic types
These are varieties that arose due to a violation of the hematopoietic function of the bone marrow and due to insufficient formation of blood cells (reduction of red blood cells, platelets and leukocytes). Hypoplastic anemia is characterized by the loss of bone tissue's ability to repair itself.
There are congenital (extremely rare) and acquired forms.
Some chemical compounds (poisonous substances, toxins), medications (including antibiotics and anti-inflammatory drugs), ionizing and X-ray radiation are to blame for the occurrence of such a disease.
Due to disruption of the hematopoietic system, infectious diseases develop, blood leaks from the nasal cavity, and hemorrhages into the mucous membranes.
Dyserythropoietic species
There is a violation of erythropoiesis (the process of formation of red blood cells). As a result, most of the nucleated cells that precede erythrocytes (pronormoblasts) die in the bone marrow, and mature erythrocytes are formed in small quantities.
The following changes are noted, which are very similar to the symptoms of hepatitis or jaundice:
- yellowness of the skin (as with hepatitis);
- enlarged liver and spleen;
- skeletal changes (high palate, tower skull, short little finger, short stature, dwarfism).
Therefore, before starting treatment, a thorough diagnosis is required.
Hemolytic anemia in children
The disease is characterized by intense destruction of red blood cells and can be hereditary or acquired during life. The hereditary type is associated with diseases such as ovalocytosis, stomatocytosis and spherocytosis. Massive damage to red blood cells occurs when they lose hemoglobin and excessive formation of bilirubin.
Cell destruction in this case occurs in the spleen. A decrease in the number of red blood cells provokes increased erythropoietic activity in the bone marrow. Symptoms of hereditary hemolytic disease can appear from birth.
These include:
- yellow skin color (due to high concentration of bilirubin);
- splenomegaly (enlarged spleen);
- unusual color of urine and feces;
- cases of anemic coma.
Factors in the development of the acquired type are malignant tumors, autoimmune connective tissue diseases, Sharp's disease, toxins entering the body, pathological structure of red blood cells (genetic disorder), malaria, toxoplasmosis, sepsis, hepatitis, Rh conflict in mother and baby.
The main classification of anemia in children also includes anemia of mixed origin (lack of several elements in the body at the same time).
Traditional methods of treatment
There are also folk methods for improving the condition of the body. You can get rid of anemia with the help of simple recipes that contain only natural and healthy products.
If you have anemia, you should try:
- "Cocktail" of juices. By mixing pomegranate, apple, carrot, beetroot and lemon juice and adding a spoonful of honey to the resulting drink, you will provide yourself with a whole set of vitamins for every day. You need to consume 2 tablespoons three times a day.
- Yarrow. Make a decoction by steaming the plant in boiling water. Keep the resulting liquid in the pan for about an hour, after wrapping it in a cloth. Take in the same way as the previous drink.
- Stewed juice. Mix beetroot, carrot juices, and black radish juice. Place the liquid in the oven for an hour, without bringing to a boil. Drink 2 tbsp. spoons half an hour before meals.
- Rowan tea. Take 2 teaspoons of berries, pour 400 ml of boiling water over them. The drink should brew for about half an hour. Drink a glass of tea twice a day. You can make rosehip tea in the same way.
These folk recipes help to consume enough vitamins every day, which helps with anemia. These methods should not be considered a panacea, so be sure to consult your doctor.
Tactics of drug therapy
Treatment of first degree anemia has several options, depending on the type of anemia. However, in all cases, the main emphasis is on replenishing iron and vitamin B12 deficiency.
Most often, high dosages of iron supplements (up to 300 mg/day) are prescribed, which are taken orally. If the hemoglobin level gradually recovers, the dose is reduced to therapeutic levels.
Modern iron preparations are often a complex of this element with vitamins B12, B9 and C.
If the patient has a malabsorption of iron due to pathology of the gastrointestinal tract, injectable forms of the drug are prescribed.
Aplastic and posthemorrhagic forms of anemia require a special approach to treatment. In the first case, therapy is aimed at restoring normal bone marrow function, so drugs are used that stimulate the division of blood cell precursors.
Only specialists can treat this type of pathology.
In the second case, blood transfusion is used in case of large blood loss. Replenishment of the normal number of red blood cells, correction of iron levels.