Mechanism of occurrence
An extrasystole is an extraordinary contraction of the heart or any part of it.
If we compare cardiac rhythm with music, then the cause of the disorder is akin to a premature erroneous note that disrupts the sound of the melody. Sometimes such failures are observed in healthy children. In the myocardium, an impulse suddenly arises not in the physiological source of excitation (sinus node), but in another area. This focus (wrong note) is so strong that it spreads through the conduction system and causes an extraordinary contraction (extrasystole), thereby disrupting the “melody of the heart.”
Kinds
Atrial extrasystoles
Often detected in healthy people with a normal heartbeat. Diagnosed mainly using 24-hour Holter monitoring in more than 60% of adults. The course of ES is often aggravated by the intake of alcohol and caffeine.
In some cases, runs of atrial ectopy can lead to paroxysms of atrial fibrillation.
Ventricular extrasystoles
Can occur at any age. More common in people with organic heart disease. Ventricular extrasystoles are the most common type of arrhythmia that occurs after myocardial infarction. They may also occur with severe left ventricular hypertrophy, hypertrophic cardiomyopathy, and congestive heart failure. According to recent studies, ventricular ES can be fatal even in the absence of any heart disease.
There are certain risks associated with ventricular extrasystoles:
- ES occurring during exercise, especially those occurring during the recovery phase, may indicate an increased risk of mortality.
- Frequent ventricular ectopies (more than 1000 per day) can adversely affect ventricular function:
- There may be slight impairment of LV function despite normal left ventricular ejection fraction.
- Frequent ventricular extrasystoles may be associated with a slow progression of decline in ventricular function (over several years or decades).
- With significant organic damage to the heart, frequent ventricular extrasystoles indicate an increased risk of sudden cardiac death.
Causes of extrasystole in children
Extrasystole can “lie in wait” for a child of any age. I have repeatedly encountered a situation where, in an apparently healthy newborn, the ECG film treacherously “shines” with one or more deformed teeth. Or, during auscultation, the symptoms of a possible extrasystole suddenly appear in a teenager. The teenager feels great and plays sports. Heart pain never bothered him.
Extrasystole is a type of arrhythmia in which extraordinary contractions (extrasystoles) are detected on the ECG. It can be congenital or acquired. Cardiac and extracardiac disorders can provoke the emergence of non-physiological foci of excitation.
Your child is at risk for heart problems if he:
- Congenital heart defect;
- rheumatism;
- cardiomyopathy;
- mitral valve prolapse.
Pediatric cardiologists separately identify arrhythmogenic dysplasia of the right ventricle as a cause of rhythm disturbances - a hereditary pathology that causes fibro-fatty degeneration of the myocardium.
Extrasystoles can be provoked by:
- endocrine diseases;
- infections;
- diseases of the nervous system;
- intoxications;
- drug overdose;
- lack of individual microelements;
- stress and emotional overstrain;
- excessive physical load;
- diaphragmatic hernia;
- diseases of the stomach and esophagus.
The etiological role of tonsillitis and adenoiditis in the pathogenesis of heart rhythm disturbances cannot be completely excluded. If extrasystoles are detected in a newborn or infant, you need to find out what the mother was sick with during pregnancy, whether there was a threat of miscarriage, whether the baby suffered intrauterine hypoxia, at what stage he was born, and whether he immediately cried. But even with detailed questioning of parents, it is not always possible to establish the cause of the pathology. We call this arrhythmia idiopathic.
Diagnostics
During development, this disease does not cause any abnormalities in the child. First of all, the doctor should talk with the baby and the parents. Children may not attach importance to periodic pain or forget about them. For a general diagnosis, the doctor evaluates the entire central nervous system.
The following studies are mandatory:
- ECG in standard form. This study allows us to identify the nature of the disease. It remains an effective tool for establishing extrasystole and other types of cardiac arrhythmias in the ventricle.
- Echocardiography. If a child has an arrhythmia due to structural changes in the heart, they are detected using this method.
- Monitoring using the Holter method. Since extrasystole in children, as a rule, has a weakly expressed short-term nature, daily monitoring and recording of cardiac activity indicators are carried out with a portable ECG. Thanks to this, it is possible to assess the child’s condition at different times of the day and the reaction to psychological and physical activity.
- Neurophysiological function is assessed.
- An analysis is carried out for intracellular infections.
- A biochemical analysis is also carried out to determine the content of electrolytes and hormone levels in the blood.
Extrasystole often occurs in conjunction with the following diseases:
- gastrointestinal dyskinesia,
- nocturnal enuresis,
- vestibulopathy,
- gastroesophageal reflux,
- biliary dyskinesia,
- increased weather dependence.
Is it necessary to further examine the child and how to do it?
Often the pathology is asymptomatic. But sometimes your son or daughter may complain of a sinking feeling inside the chest, sudden sharp pain in the chest, temporary cardiac arrest, and then a sharp blow against the chest wall. It should be understood that the baby cannot always express complaints. One day, a five-year-old boy, pointing to his chest, described his condition to me this way: “There is a ball there, and it sometimes bounces painfully.”
In adolescents, extrasystoles are sometimes accompanied by dizziness, weakness, and a feeling of lack of air. The mother of a child in his first year of life may notice periodic bouts of anxiety, poor sleep, and breast refusal.
ECG changes
It is necessary to further examine a child with suspected or accidentally detected extrasystole in order to exclude organic heart pathology and decide on further tactics. The main diagnostic method is electrocardiographic examination. It is carried out at rest and after physical activity. The film may contain one extrasystole or several.
Depending on the location of the source of excitation, extrasystoles are distinguished:
- supraventricular;
- ventricular;
- atrioventricular (atrioventricular).
I advise you to definitely conduct Holter monitoring for your child - recording an ECG throughout the day with a portable device. At this time, let the baby lead a normal life. Such an examination will allow:
- determine the circadian rhythm of extrasystole (depending on the time of day);
- identify the connection between the appearance of pathological foci of excitation and physical activity;
- assess the incidence of extrasystoles.
Do not be surprised if the doctor prescribes Holter monitoring for your child in the absence of extrasystoles. Perhaps this particular method will help “catch” a premature contraction that could not be recorded on a regular electrocardiogram.
Additional examinations
It is important to find out the cause of the non-physiological impulse. Clinical recommendations for the management of children with ventricular extrasystoles, approved by the Association of Pediatric Cardiologists and the Union of Pediatricians of Russia, suggest performing the following auxiliary examinations:
- biochemical blood test - will exclude myocarditis and possible electrolyte imbalance;
- determination of thyroid hormones - if hypo- or hyperthyroidism is suspected;
- echocardiography – will make it possible to assess structural changes in the heart, the condition of the myocardium, and the size of the chambers;
- magnetic resonance imaging of the heart - recommended for suspected arrhythmogenic dysplasia of the right ventricle.
To clarify the diagnosis, a pediatric cardiologist can refer a small patient to transesophageal electrocardiography, electroencephalographic examination, consultation with a geneticist or other specialized specialists.
What is supraventricular extrasystole?
Extrasystole is the general concept of extraordinary (arrhythmic) heart contractions. According to localization they are divided into the following types:
- supraventricular extrasystole (supraventricular);
- ventricular extrasystole (ventricular);
- antiventricular extrasystole (atrioventricular).
The foci of supraventricular extrasystoles are located in the atria, that is, above the ventricles. Hence the name arrhythmia. The atrioventricular form is characterized by the appearance of ectopic (arising in the wrong place) contractions in the septum between the atrium and the ventricle or between the ventricles. Ventricular extrasystole is localized in the ventricles. The consequence of supraventricular and ventricular extrasystoles is often changes in the muscle tissue of the heart (myocardium).
Classification of atrial extrasystole is made according to many parameters. By number of pulses per minute:
- single (number of unscheduled layoffs 1 - 5);
- paired (two pulses in a minimum period);
- group (several reductions per period);
- multiple (over 5 extraordinary impulses).
Based on the number of sources of impulse generation, they are distinguished between monotypic (one source) and polytopic (more than one source of excitation). If there is a certain pattern in the passage of normal contractions and extraordinary ones, then they speak of organized extrasystole. If this alternation is chaotic, then it is called disorganized. Division by etiology (origin) of arrhythmia:
- organic extrasystole is caused by pathological changes in the heart, which in particular includes sinus extrasystole;
- functional, resulting from other disorders in the body.
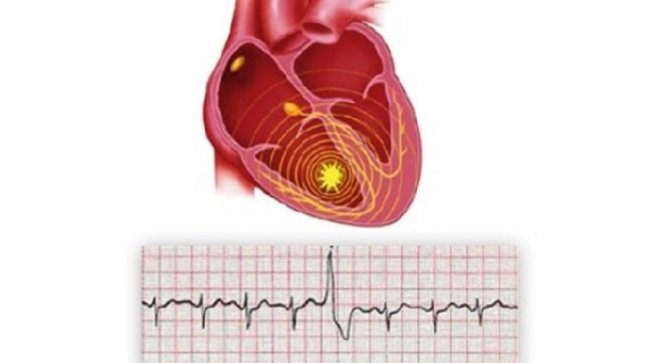
Extrasystole on an ECG
Extrasystole leads to the fact that the heart cannot fully contract. And this in turn can cause supraventricular tachycardia and fibrillation.
In what cases should it be treated and with what methods?
At the moment, there is no single protocol for the treatment of extrasystole in children. The cardiologist selects therapy individually, depending on the location of the non-physiological focus, the frequency of altered complexes, age, subjective feelings of the child, and the presence of hemodynamic disorders. If the cause for your baby is established, we focus on eliminating it and treating the underlying disease.
Quite often it is difficult for parents to come to terms with the fact that the doctor does not prescribe medications. Believe me: with single ventricular extrasystoles and no complaints, the condition is not dangerous. Such children need a medical examination at least once a year.
According to the Framingham study, if there are accompanying clinical symptoms, Holter monitoring should be performed annually, as there is a possibility of persistence or transformation of extrasystole into a more serious cardiovascular pathology.
Try to explain to your son or daughter what is necessary to maintain health:
- maintain a sleep and rest schedule;
- learn to cope with stress;
- give up fast food, eat foods rich in potassium, magnesium, selenium, and vitamins;
- get vaccinated in a timely manner.
It is important to discuss the dangers of bad habits with a teenager in a simple and accessible manner. The issue of exemption from physical education lessons is decided individually. Extrasystoles in the neonatal period do not require special therapy. Try to breastfeed your baby for as long as possible and follow all the recommendations of your pediatrician.
Medicines are prescribed to restore sinus rhythm. The medicine is selected strictly for a particular child. It is often sufficient to use drugs containing potassium and magnesium that improve cellular metabolism, sedatives, anticonvulsants, and antidepressants.
Sometimes the child is prescribed antiarrhythmic drugs. Usually - with a supraventricular (supraventricular) form of extrasystole.
One of the ways to combat extrasystole is to perform radiofrequency catheter ablation - insertion of an electrode through large vessels into the cardiac cavity, with the help of which the zone of the pathological impulse is destroyed. Rarely used in children.
Prevention
To prevent the occurrence of extrasystoles, it is important to avoid violations of the daily routine, severe psycho-emotional and physical overload, and bad habits. Effective measures to prevent extrasystole are:
- Balanced diet.
- Daily walks.
- Favorable psychological climate.
- Sufficient sleep duration.
- Timely treatment of any pathologies.
- Moderate physical activity.
- Strengthening protective forces.
Cardiac activity is a very complex process. The heart is wrapped in nerve pathways, like wires. Thanks to them, the heart muscle contracts. The conduction system sets the heart rhythm, which must be correct. This means that the same number of seconds should pass between heartbeats. But it happens that the heartbeat gets confused and arrhythmias occur. In our article we will talk about the most common type of arrhythmia - extrasystole.
Extrasystole is premature excitation of the myocardium. It can be in both the ventricles and atria.
Forecast: is it worth worrying about?
If a cardiologist has announced that your child has extrasystole, I advise you not to panic, but to clarify the cause of the disturbances with your doctor and discuss further tactics. Recovery will most likely not occur. Sometimes extrasystoles spontaneously disappear and do not appear for several years, and then suddenly appear again on the ECG.
Ventricular extrasystoles in the absence of clinical manifestations are not an obstacle to exercise in the sports section. If you follow medical recommendations, the patient can lead an active lifestyle and maintain full working capacity for many years.
Symptoms
Supraventricular extrasystoles are insidious in that they often do not have any pronounced symptoms.
Patients often do not have any complaints, and the disease proceeds unnoticed, but only for some time.
Supraventricular extrasystole may have the following symptoms:
- Shortness of breath, feeling of suffocation.
- Dizziness (this occurs due to decreased blood flow and oxygen starvation).
- Weakness, increased sweating, discomfort.
- Interruptions in the work of the heart (feeling of beats outside the heart).
- “Hot flashes” that have no reason.
The most important and common sign of the disease is a feeling as if the heart stops for a while. Most often this causes panic, anxiety, paleness, etc. in people.
Generally speaking, supraventricular extrasystole accompanies a large number of heart diseases. Sometimes it is associated with the presence of vegetative or psycho-emotional disorders.