Difference between bypass and stenting
Sometimes, with heart problems, the condition becomes so serious that conventional medications no longer help.
In such cases, you have to resort to some radical methods to improve the situation. Let's look at two options for surgical intervention and find out how bypass surgery differs from stenting. The condition of the heart depends on the quality of its blood supply. And this, in turn, is determined by the degree of vascular patency. When everything is in order, they have smooth walls, and the blood moves without stopping along the right path. But over time, the vessels in some places can become very narrow and become overgrown with atherosclerotic deposits.
All this disrupts blood flow. The tissues of the main organ begin to experience oxygen starvation. The logical consequence in such a situation is the development of cardiac ischemia. Complete blockage of the vessel is especially dangerous. In an area deprived of blood supply, the tissue dies and myocardial infarction occurs. The operations in question make it possible to prevent such an outcome, and sometimes even save the life of a person already in critical condition.
The goal of both interventions is to normalize blood flow. However, the result in each case is achieved in its own way. Considering the difference between bypass surgery and stenting, it is worth noting that the second of these operations is easier and is often performed faster.
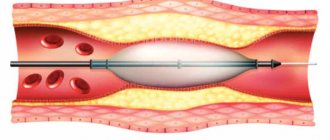
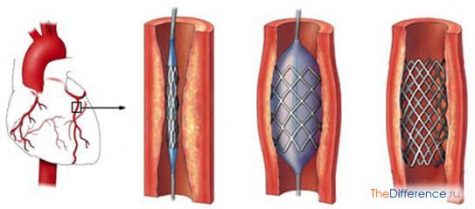
Stenting be put under anesthesia. The essence of the procedure is to expand the problem area of the vessel by installing an implant. To do this, a puncture is made in the area of the femoral artery under local anesthesia. Through this slot, a long narrow tube is inserted into the vessel. At its end there is a deflated balloon, on top of which a stent is fixed, also compressed.
The structure is advanced through the artery under X-ray control and brought to the affected area. After this, the can is inflated. Inflating, it causes the stent to expand and firmly fix itself in the form of a flexible tubular mesh in the walls of the vessel. Then all the auxiliary instruments are removed, and only the implant remains in the body, which subsequently prevents the lumen from narrowing and ensures the normal passage of blood.
Stenting
Bypass surgery is a more complex and risky operation, but is nevertheless sometimes necessary. Such intervention is performed when the installation of a stent is futile or impossible. This method is used, for example, when the diameter of the affected vessel is miniature, in the case of atherosclerotic changes of a large extent, or when multiple blockages of the lumens are detected.
Here, the meaning of the surgical actions is to create an artificial blood flow path using a shunt. In this case, the blocked part of the vessel is excluded from the circulation system. The shunt most often becomes a fragment of a vein or artery from another area of the body. In some cases, artificial materials are used.
Bypass surgery
To restore blood flow in this way, an incision is made in the chest area. The person being operated on is under anesthesia. Bypass surgery is often performed on a non-functioning heart, while providing artificial circulation. If possible, make do with small incisions in the intercostal spaces.
What is the difference between bypass surgery and stenting? It also lies in the terms of rehabilitation after the actions taken. In the first case, the recovery period lasts longer, in the second, the patient usually gets back to his usual routine faster. In addition, bypass surgery entails many more possible limitations in the future than stenting.
Source: thedifference.ru
General information
The condition of the heart depends on the quality of its blood supply. And this, in turn, is determined by the degree of vascular patency. When everything is in order, they have smooth walls, and the blood moves without stopping along the right path. But over time, the vessels in some places can become very narrow and become overgrown with atherosclerotic deposits.
All this disrupts blood flow. The tissues of the main organ begin to experience oxygen starvation. The logical consequence in such a situation is the development of cardiac ischemia. Complete blockage of the vessel is especially dangerous. In an area deprived of blood supply, the tissue dies and myocardial infarction occurs. The operations in question make it possible to prevent such an outcome, and sometimes even save the life of a person already in critical condition.
Comparison of operations: results of clinical studies
Over the past three years, several serious scientific papers have been published, summarizing the results of clinical studies that were conducted in a group of patients with cardiovascular diseases and studied the effectiveness and safety of various treatment methods.
The results of the first study, called Syntax, were published in the Lancet in February 2013. The study was carried out in a group of 1800 patients with stenosis of the three main coronary arteries or stenosis of the common left coronary artery. Half of the patients underwent coronary artery bypass surgery, and the other half had a new generation drug-eluting stent installed. In terms of the severity of the clinical condition, both groups were identical. Based on the results of a 5-year observation, the researchers came to the following conclusions:
Data collected in the
second study (Freedom) were published in the New England Journal of Medicine (NEJM) in December 2012. This time, a comparative analysis of the effectiveness of stenting using new generation stents and coronary artery bypass grafting was carried out among patients with diabetes mellitus .
It is a well-known fact that stenting in patients with diabetes is often accompanied by restenosis of the coronary arteries. The reason for this phenomenon lies in abnormalities of the vascular wall that develop as a result of diabetes mellitus. Until now, there was no reliable information about the effectiveness of using new generation stents in this category of patients. The results of the Freedom study brought final clarity to this issue. Five-year observation was carried out over two groups of patients, each of which consisted of 950 people. The researchers came to the following conclusions: The researchers concluded that in patients with diabetes, coronary artery bypass grafting is a more effective and safer procedure than stenting, even when drug-eluting stents are used.
The third study (Ascert) , the results of which were published in March 2012 in NEJM, is rightfully considered one of the most large-scale in the history of cardiology and cardiac surgery. Its organizers used the information base of the American professional societies of cardiologists and thoracic surgeons (ACC - American College of Cardiology, STS - Society of Thoracic Surgeons) for 2004-2008. The information database contains data on more than 2 million patients in the United States who underwent either stent implantation or coronary artery bypass surgery during the reporting period. The final sample included 190,000 clinical cases. The patients were observed for 4 years. The postoperative mortality rate in the group after coronary artery bypass surgery was 16.4%, in the group of patients who underwent stent installation - 20.8%. In other words, the mortality rate among patients in whom coronary artery bypass grafting was chosen as a treatment method was 21% lower compared to those in whom stent implantation was performed.
Which is better - CABG or stenting?
Only a cardiac surgeon can answer this question regarding each specific patient with angina during an in-person examination . However, some benefits have been identified for both treatments.
Thus, stenting is characterized by a less traumatic operation, better tolerance by patients, and no need for general anesthesia. In addition, the patient spends fewer bed days in the hospital and can start working earlier.
Bypass surgery is performed using one’s own tissues (veins or arteries), that is, there is no foreign body in the body. Also, the likelihood of re-stenosis of a bypass is lower than that of a stent. If the patient has diffuse damage to the coronary vessels, bypass surgery can solve this problem, unlike a stent.
So, in conclusion, I would like to note that despite the fact that many patients are wary of the possibility of heart surgery, they should listen to the recommendations of the attending physician and, if stenting is necessary, they should give their thoughts a positive attitude and boldly go for the operation. Moreover, over decades of successful operations on coronary vessels, doctors have been able to accumulate a sufficient evidence base indicating that stenting reliably prolongs life and reduces the risk of developing myocardial infarction.
operaciya.info
Combining coronography with angioplasty and stenting is undesirable
In most situations, according to leading experts, it is undesirable to combine coronary angiography, which is a diagnostic procedure , with therapeutic procedures: angioplasty and stenting. If coronary angiography diagnoses coronary artery stenosis, but the patient's condition does not require emergency medical care, it is not recommended to immediately proceed to angioplasty and stent placement. The decision to choose a technique should be made collectively, after careful discussion of all aspects of the procedure, while respecting the patient's rights to participate in the treatment process and obtaining informed consent.
Currently, American and European associations of doctors specializing in the treatment of cardiovascular pathologies recommend using the Heart Team concept in clinical practice. The team should be composed of both cardiologists and cardiac surgeons, and consider each clinical case individually. This is how strategic decisions are made at the Herzliya Medical Center private clinic when it comes to treating patients with serious cardiovascular diseases.
Source: hmc-israel.org.il
Preparation and performance of the operation
Stenting can be performed urgently or routinely. In emergency surgery, coronary angiography (CAG) is first performed, based on the results of which a decision is immediately made to introduce a stent into the vessels. Preoperative preparation in this case comes down to the introduction of antiplatelet agents and anticoagulants into the patient’s body - drugs that prevent increased blood clotting (to avoid thrombosis). As a rule, heparin and/or clopidogrel (warfarin, Xarelto, etc.) are used.
Before a planned operation, the patient must perform the necessary research methods to clarify the degree of vascular damage, as well as assess the contractile activity of the myocardium, the ischemic zone, etc. For this, the patient is prescribed CAG, ultrasound of the heart (echocardioscopy), standard and stress ECG, transesophageal electrical stimulation myocardium (TEFI - transesophageal electrophysiological study). After all diagnostic methods have been completed, the patient is hospitalized in the clinic where the operation will be performed.
The evening before the operation, a light dinner is allowed. It is likely that some cardiac medications will need to be discontinued, but only as directed by the attending physician. Breakfast before surgery is not allowed.
Stenting itself is performed under local anesthesia. General anesthesia, dissection of the chest and sternum, and connection of the heart to a heart-lung machine (ACB) are not required.
At the beginning of the operation, local anesthesia of the skin is performed in the projection of the femoral artery, which is accessed through a small incision. An introducer is inserted into the artery - a conductor, through which a catheter with a stent installed at the end is brought to the affected coronary artery. Under the control of X-ray equipment, the exact position of the stent at the site of stenosis is monitored.
Next, the balloon, which is always inside the stent in a compressed state, is inflated using air injection, and the stent, being a spring structure, is straightened out, tightly fixed in the lumen of the artery.
After this, the catheter with the balloon is removed, a tight aseptic dressing is applied to the skin incision, and the patient is transferred to the intensive care unit for further observation. The entire procedure lasts about three hours and is painless.
After stenting, the patient is observed for the first day in the intensive care unit, then transferred to a regular ward, where he remains for about 5-7 days until discharge from the hospital.
Video: stenting, medical animation
Indications for surgery
If you are registered with a cardiologist, suffer from hypotension, or experience one of the following conditions, you may be recommended to undergo coronary stenting:
- An increase in the ST interval on the cardiogram (indicates a heart attack or microinfarction of the heart muscle).
- With unstable angina or increased frequency of attacks with increased pain, accompanied by arrhythmia.
- Identified pre-infarction state.
- Angina pectoris, which is poorly treated with medication.
- With poor effectiveness of coronary artery bypass grafting.
Coronary stenting (heart vessels)
- What is a “stent” and its types
- How is the operation performed?
- Indications for surgery
- Contraindications
- Complications
- Rehabilitation
The main cause of the most serious manifestation of coronary heart disease, myocardial infarction, is a malnutrition of the muscle due to atherosclerotic vascular damage.
Atherosclerosis affects the artery wall. Due to loss of elasticity, the possibility of sufficient expansion is lost. The deposition of atherosclerotic plaques from the inside causes a narrowing of the diameter of the vessel and impedes the delivery of nutrients. A critical reduction is considered to be 50% of the diameter. At the same time, clinical symptoms of hypoxia (lack of oxygen) of the heart begin to appear. This is expressed in attacks of angina pectoris.
Complete blockage of the coronary artery leads to the development of an area of necrosis (necrosis) during myocardial infarction. Throughout the world, this pathology is still considered one of the main causes of death in adults.
Timely stenting of cardiac vessels helps prevent the development of severe complications of atherosclerosis.
What is "stenting"?
The term “stenting” refers to the operation of installing a stent inside an artery, which results in mechanical expansion of the narrowed part and restoration of normal blood flow to the organ. The operation refers to endovascular (intravascular) surgical interventions. It is carried out in vascular departments. It requires not only highly qualified surgeons, but also technical equipment.
In surgery, methods have been established not only for coronary stenting (heart vessels), but also for installing stents in the carotid artery to eliminate signs of cerebral ischemia, in the femoral artery to treat atherosclerotic changes in the legs, in the abdominal aorta and iliac artery in the presence of pronounced signs of atherosclerotic lesions.
What is a “stent”, types
A stent is a lightweight mesh tube that is strong enough to provide a framework for the artery for a long time. Stents are made from metal alloys (usually cobalt) in accordance with high technology. There are many types. They differ in size, mesh structure, and type of coating.
There are two groups of stents:
- without coating - used for operations on medium-sized arteries;
- covered with a special polymer shell that releases a medicinal substance throughout the year that prevents re-stenosis of the artery. The cost of such stents is much more expensive. They are recommended for installation in coronary vessels and require constant use of medications that reduce the formation of blood clots.
How is the operation performed?
To stent the heart vessels, a catheter is inserted into the femoral artery, at the end of which there is a tiny balloon with a stent placed on it. Under the control of an X-ray machine, the catheter is inserted into the mouth of the coronary arteries and moved to the desired area of narrowing. The can is then inflated to the required diameter. In this case, atherosclerotic deposits are pressed into the wall. The stent expands like a spring and remains in place after the balloon is deflated and the catheter is removed. As a result, blood flow is restored.
The operation is usually performed under local anesthesia. Lasts from one to three hours. Before surgery, the patient is given blood thinning medications to prevent thrombosis. If necessary, several stents are installed.
After surgery, the patient spends up to seven days in the hospital under the supervision of a doctor. He is advised to drink plenty of fluids to eliminate contrast agents in the urine. Anticoagulants are prescribed to prevent platelets from sticking together and forming blood clots.
Who is indicated for surgery and examination?
The selection of patients with coronary heart disease for surgical treatment is carried out by a consultant cardiac surgeon. In the clinic at the place of residence, the patient undergoes the necessary minimum examination, including all mandatory blood and urine tests to determine the functioning of internal organs, a lipogram (total cholesterol and its fractions), and blood clotting. Electrocardiography allows you to clarify the areas of myocardial damage after a heart attack, the extent and localization of the process. Ultrasound examination of the heart clearly shows the functioning of all parts of the atria and ventricles.
In the inpatient department, angiography is mandatory. This procedure involves the intravascular injection of a contrast agent and a series of x-rays taken as the vascular bed fills. The most affected branches, their location and the degree of narrowing are identified.
Intravascular ultrasound helps evaluate the capabilities of the artery wall from the inside.
The examination allows the angiosurgeon to determine the exact location of the proposed stent insertion and identify possible contraindications to the operation.
Indications for surgery:
- severe frequent attacks of angina, defined by a cardiologist as a pre-infarction condition;
- support for aortocoronary bypass (bypass is the installation of artificial blood flow to bypass a blocked vessel), which tends to narrow within ten years;
- for health reasons in severe transmural infarction.
Contraindications
The impossibility of stent insertion is determined during the examination.
- Widespread disease of all coronary arteries, due to which there is no specific site for stenting.
- The diameter of the narrowed artery is less than three mm.
- Reduced blood clotting.
- Impaired kidney and liver function, respiratory failure.
- Allergic reaction of the patient to iodine drugs.
The advantage of stenting over other operations:
- low invasiveness of the technique - there is no need to open the chest;
- short period of patient stay in hospital;
- relatively low cost;
- rapid recovery, return to work, absence of long-term disability for the patient.
Complications of the operation
However, 1/10 of those operated on had complications or undesirable consequences:
- perforation of the vessel wall;
- bleeding;
- formation of blood accumulation in the form of a hematoma at the puncture site of the femoral artery;
- stent thrombosis and the need for re-stenting;
- renal dysfunction.
Video clearly showing the essence of the operation:
Recovery period
Stenting of the heart vessels can significantly improve the patient’s well-being, but this does not stop the atherosclerotic process or change the impaired fat metabolism. Therefore, the patient will have to follow the doctor’s orders and monitor cholesterol and blood sugar levels.
You will have to exclude animal fats from your diet and limit carbohydrates. It is not recommended to eat fatty pork, beef, lamb, butter, lard, mayonnaise and spicy seasonings, sausages, cheese, caviar, pasta from non-durum wheat, chocolate, sweets and baked goods, white bread, coffee, strong tea, alcohol and beer, carbonated sweet drinks.
The diet requires that you include vegetables and fruits in salads or fresh juices, boiled poultry, fish, cereals, durum pasta, cottage cheese, fermented milk products, and green tea.
It is necessary to establish 5-6 meals a day and monitor your weight. If necessary, carry out fasting days.
Daily morning exercises increase metabolism and improve mood. You can’t take on heavy exercises right away. Walking is recommended, first for short distances, then increasing the distance. Slow walking up the stairs is popular. You can exercise on exercise machines. Patients should definitely learn to count their pulse. Avoid significant overload with increased heart rate. Sports recommended include cycling and visiting the pool.
Drug therapy is limited to drugs that lower blood pressure (in hypertensive patients), statins to normalize cholesterol levels, and drugs that reduce blood clots. Patients with diabetes should continue specific treatment as prescribed by the endocrinologist.
It is better if rehabilitation after stenting is carried out in a sanatorium-resort environment, under the supervision of doctors.
Stenting surgery has been performed for about forty years. The methodology and technical support are constantly being improved. The indications are expanding, there are no age restrictions. It is recommended that all patients with coronary heart disease not be afraid of consulting a surgeon; this is an opportunity to prolong their active life.
What is stenting?
Coronary stenting is also called “transluminal percutaneous coronary angioplasty with stenting.” This is a procedure for installing a special stent inside a vessel in order to expand its lumen and restore normal blood supply.
A stent is a metal mesh tube of different lengths and diameters. They are made from various metal alloys, based on cobalt. There are two types:
- Uncoated stents are small or medium diameter stents that are installed in small vessels.
- Coated with polymer – used for coronary stenting. The coating contains medications that prevent the re-growth of atherosclerotic plaques inside the vessel, relieve inflammation, and prevent the growth of the muscle layer. Such a stand costs much more. After its installation, the patient must be under medical supervision and constantly take medications to thin the blood.
- Coated with precious metals. Titanium, silicon, gold, and carbon are used. They are used to ensure that the coating does not react with the tissues of the vessel and blood.
- Biosoluble or absorbable - disappear after 1-1.5 years, releasing drugs that prevent vasoconstriction.
The type of mesh can also be different and is selected depending on the type of vessel where it will be installed. Stents are installed not only in the vessels of the heart, but also in the carotid, femoral, iliac, and abdominal arteries. This allows you to fight thrombosis of the veins of the lower extremities, cerebral ischemia and other atherosclerotic lesions.
The operation is considered endovascular and low-traumatic. To perform it, you do not need to open the chest and make large incisions, which means the recovery period is shorter and easier.
In which cases is it better to do bypass surgery, and in which stenting?
All of the listed pros and cons of both types of cardiac intervention and their differences play a minor role in the choice of surgical treatment method. Bypass or stenting is decided by the doctor after a comprehensive assessment of the patient’s condition, in particular the vessels of his heart. For this purpose, the SyntaxScore is used, which determines more effective and less dangerous tactics. Especially with complex lesions or atherosclerotic stenosis of the trunk of the left coronary artery.
Whatever operation is prescribed, the course of the postoperative period depends on the patient’s strict compliance with the doctor’s instructions. This includes taking medications, following a diet, and doing daily exercise. Consequently, the duration and fullness of life after stenting or bypass surgery depends on the patient himself.
Source: holestein.ru
Is stenting or bypass surgery better – what do experts say?
Coronary heart disease (CHD) is a real problem for humanity in the 21st century. Poor nutrition and a sedentary lifestyle lead to excess cholesterol forming atherosclerotic plaques on blood vessels, significantly impairing blood flow. The most dangerous thing for the “proper” functioning of the heart is the narrowing of the lumen in large arteries. Insufficient oxygen supply to the myocardium is one of the reasons for the development of coronary artery disease. Thanks to the latest methods of treating heart disease, it has become possible to improve the condition of patients suffering from coronary artery disease. Such procedures today are stenting and bypass surgery of large vessels, after which it is possible to fully restore oxygen supply to the heart, but it is clear that specialists have not been able to do better for many years.
Many of our readers actively use a well-known method based on natural ingredients, discovered by Elena Malysheva, to treat HEART DISEASES. We recommend that you check it out.
Despite some disagreements among surgeons and cardiologists, both methods of restoring vascular patency have been demonstrating good performance in the treatment of coronary artery disease for a long time. But still, each of them differs in the way the procedure is carried out, and also has its own advantages and disadvantages. We'll look at which ones next.
If you have any additional questions, our experienced specialists will be able to advise you free of charge.
Just enter your question in the pop-up form.
Complications of cardiac artery stenting
Unfortunately, with stenting, like any other surgical intervention, complications are possible. The following conditional division of these complications is accepted: Intraoperative complications, i.e. arising during the operation:
- Heart rhythm disturbances
- Myocardial infarction
- Vessel dissection, i.e. detachment of the inner lining of the artery
- Angina attack
- In rare cases, death can occur.
Rarely, but it is possible for a situation to develop in which a transition from stenting to coronary artery bypass surgery is possible.
- Heart rhythm disturbances
- Stent thrombosis, with possible development of myocardial infarction
- Hematoma at the puncture site
- True or false aneurysm of the punctured artery
Late postoperative complications
Stenting or bypass surgery – which is better and more reliable?
One of the modern methods of restoring vascular patency is stenting and bypass surgery. These procedures are most often used in the case of coronary heart disease, when the coronary arteries that supply the heart muscles become blocked by atherosclerotic plaque at a certain interval.
During stenting, a special metal structure in the form of a mesh is installed into the lumen of the vessel, which eliminates the narrowing. With bypass surgery, a bypass for blood flow is performed when the donor vein or the patient’s vein is sutured above and below the site of narrowing. Both operations performed by Israeli surgeons are effective, but have their advantages and disadvantages.