Quite often in medicine there are situations when the fact of the presence of deviations from standard indicators is determined by chance during routine examinations, undergoing a full examination for surgical other types of interventions. As a rule, such pathologies are asymptomatic for a long time, but this is precisely the main danger to humans.
By upsetting the balance in the functioning of the body's systems and causing a chain reaction of changes, often irreversible, the disease manifests itself during the peak of its development. In this edition we will talk about the circulatory system of the body, or more precisely about the aorta.
During an ultrasound of the heart, the doctor may use the term “the aorta is thickened,” not every person knows what this means and what it can lead to.
Complete blood circulation depends on the condition of the blood vessel system.
Compaction, as well as other types of vascular deformation, impair blood flow, which performs a number of important functions in addition to supplying the body with oxygen, namely:
- nutrient enrichment;
- delivery of hormones to organs;
- transfer of metabolic products to neutralizing and excretory organs.
Considering the connection of the cardiovascular system with the entire body, when there are disturbances in its functioning, absolutely all organs and systems are affected, since they need constant nutrition, as well as cleansing. However, the person’s heart suffers first, as a result of which, as a rule, more obvious symptoms begin to appear.
To clarify the diagnosis and collect a complete picture of the disease, the consequence of which is compaction, a consultation with a cardiologist, a number of additional studies, and laboratory tests are necessary.
Causes of thoracic aortic aneurysm
The cause of a thoracic aortic aneurysm is weakness of its wall, which is why blood literally squeezes out a protrusion sac in its wall. In turn, the following factors can lead to weakness of the aortic wall:
- mechanical;
- pathological.
Mechanical factors are:
- external injuries of the aorta - under the influence of a non-medical factor;
- Iatrogenic injuries – damage to the orta during diagnostic and therapeutic procedures (operations);
- poor-quality suture material used during surgery on the aorta;
- low-quality aortic prostheses previously installed.
Pathological factors include:
- inflammatory;
- exchange. Usually this is atherosclerosis - the accumulation of cholesterol on the inner surface of the vessel, which leads to a decrease in its diameter;
- infectious – infection by bacteria, protozoa, fungi, and so on.
Please note:
Aortic aneurysm can occur as a result of intrauterine development disorders. The reason for this is aggressive factors affecting the pregnant woman, and therefore the fetus - physical, chemical, infectious, bad habits of the expectant mother and others.
Development of pathology
Several varieties of the described pathology have been identified - this is an aneurysm:
- ascending aorta;
- arcs;
- descending aorta;
- sinus of Valsalva - at the root of the aorta, where it departs from the chambers of the heart.
Normally, in adults, the diameter of the ascending aorta is 3 cm, and the descending aorta is 2.5 cm. If it is greater than these values, then an aneurysm of the affected part of the thoracic aorta is diagnosed.
In all cases, the principle of the formation of an aneurysmal protrusion is the same: blood presses on the weakened wall of the thoracic aorta and “squeezes out” a pocket in it, which becomes deeper over time.
What is the aorta and where is it located?
The aorta is considered the largest vessel of the body and has a key role in maintaining normal hemodynamics. It is from here that a large circle of blood circulation begins, which supplies oxygen-rich blood to all structures of the body. It departs from the left ventricle of the heart, is mostly located along the spinal column and ends, diverging into two branches: the right and left iliac.
Structure and departments
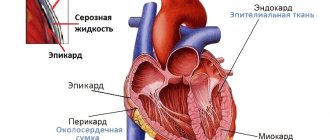
It belongs to the elastic type of arteries; histologically its wall is formed by three layers:
- Internal (intima) – represented by endothelium. It is he who is most susceptible to pathological processes, including atherosclerosis. This lining forms the aortic valve.
- Middle (media) - mainly consists of elastic fibers, which, when stretched, increase the lumen of the bed. This allows you to maintain stable blood pressure. It also contains a small amount of smooth muscle fibers.
- External (adventitia) - consists mainly of connective tissue elements with a low content of elastic fibers and high collagen, which gives the vessel additional rigidity, despite the small thickness of the wall.
Topographically, the artery consists of three main parts: the ascending section, the arch and the descending section.
The ascending section begins in the area of the third intercostal space, along the left edge of the sternum. The aortic valves are located at the point where the vessel exits the heart. Their second name is “crescentic” because they resemble curved pockets, consisting of three leaflets and preventing the reverse flow of blood after the aorta has left the ventricle. There are also small bulges - sinuses, in which the coronary arteries that supply the myocardium begin. In the same place there is a short expanded section - the bulb. Opposite the articulation of the second right rib with the sternum, the ascending aorta passes into the arch.
The arc turns to the left and ends near the fourth thoracic vertebra, forming the so-called isthmus - a place where the artery is somewhat narrowed. Posterior to this is the tracheal bifurcation (the point at which the breathing tube divides into two bronchi). Branches extending from its upper side supply the upper part of the body:
- brachiocephalic trunk;
- left general carotid;
- left subclavian.
The descending section is the longest part of the vessel, consisting of the thoracic (thoracic) and abdominal (or abdominal) sections. It originates from the isthmus of the arch, is mostly located in front of the spine and ends near the fourth lumbar vertebra. At this point, the aorta diverges into the right and left iliac branches.
The thoracic region is located in the thoracic cavity and extends to the aortic opening of the respiratory muscle of the diaphragm (opposite the 12th vertebra). Along its entire length there are branches that supply blood to the organs of the mediastinum, lungs, pleura, muscles and ribs.
The final, abdominal part, provides blood supply to the abdominal and pelvic organs, the abdominal wall, and the lower extremities.
Normal vessel size indicators
Determining the diameter of the aorta is very important in the diagnosis of many of its pathologies, especially aneurysms or atherosclerosis. This is usually done using x-ray (for example, computed tomography or magnetic resonance imaging) or ultrasound (echocardiography) studies. It is important to remember that this value is very variable, as it changes depending on age and gender.
| Department | Diameter, cm | |
| Men | Women | |
| Root | Blood flow, speed and pressure | |
Also, to study the work of the aorta, its functional indicators are examined. This is usually done using ultrasound or Doppler ultrasound.
Systolic pressure in the vessel is about 120-140 mmHg. Art., diastolic – 70-90 mm Hg. Art. The value may vary slightly depending on age and individual characteristics.
The linear speed of blood flow in the initial sections is about 0.7-1.3 m/s. Distally (i.e. further from the beginning) it decreases to 0.5 m/s.
The normal flow rate is 4-5 liters per minute.
Symptoms of a thoracic aortic aneurysm
Often there are no signs of pathology until complications occur. The “silence” of an aneurysm is a problem in cardiac surgery - people do not know about it until complications arise that pose a threat not only to the health, but also to the life of the patient.
If symptoms occur, they largely depend on which segment of the thoracic aorta is affected.
With an aneurysm of the ascending aorta, the following occurs:
- pain in the heart or behind the sternum;
- a growing feeling of lack of air;
- heartbeat;
- cerebral signs – dizziness, headaches.
note
Indicative is the so-called vena cava syndrome - swelling of the soft tissues of the face and upper chest, which occurs due to the fact that the aneurysm presses on the superior vena cava.
With an aortic arch aneurysm, the following appears:
dysphagia (difficulty swallowing);
- change in voice (hoarseness);
- in some cases - coughing;
- increased salivation;
- dyspnea.
With an aneurysm of the descending aorta, the following occurs:
- pain in the upper left limb and shoulder blade;
- loss of sensation in this area;
- disturbance of movements in the hand;
- radicular type pain in the thoracic and lumbar back.
Aortic arch
In acute dissection, the aortic arch usually has a normal or near-normal diameter, often with evidence of subadventitial hemorrhage and edema, as does the ascending aorta. In chronic dissection, the arch may be captured by aneurysmal dilatation along with the ascending and descending sections. There may be signs of arch perforation, which is usually recognized by a massive hematoma in the mediastinum. Within the arch, the dissection covers various portions around the circumference of the aorta, while the portion facing the pulmonary artery usually remains intact.
In the absence of a primary defect in the ascending aorta, it is usually found in the arch, and is often localized at the origin of the innominate artery, which is important in relation to the type and extent of the required replacement.
The dissection may stop at the origin of the arch branches, leaving them undissected. Typically, one or even all branches of the arch arise from the true aortic canal with noncircular dissection extending to varying degrees along their course, sometimes with lumen communications at the periphery. Cases when the true lumens of one, two or all supra-aortic vessels are torn at their origins and thereby form secondary messages are rare, but are of particular surgical significance. The inner wall of the arch branches may then invaginate distally, leading to vascular occlusion.
Although supra-aortic branch dissection was a common finding reported by Hirst, neurological symptoms were observed in only 19% of patients who died from dissection. Neurological deficits were frequently observed in the Pate clinical trial, where 15% of patients had cerebral impairment and 6% had paraplegia. The corresponding figures, according to DeBakey, were 9% and 2%. In the Cambria series, 43 of 325 patients (13%) had involvement of the supra-aortic branches, and 9% of them were symptomatic.
Diagnosis of thoracic aortic aneurysm
The diagnosis is made based on the patient’s complaints, details of the anamnesis (history of development) of the pathology, and the results of additional examination methods.
When studying the anamnesis, the following details are revealed:
- whether the patient has been diagnosed with infectious pathologies accompanied by various complications;
- whether the patient suffered chest injuries;
- whether he had any surgical interventions on the chest organs
A physical examination reveals the following:
- upon examination, the general condition is satisfactory; in patients with an asthenic body type, pulsation of the chest wall may be observed;
- during palpation (palpation) – when covering the patient’s chest with both hands, the examiner may feel a slight vibration provoked by the pulsation of the aneurysm;
- during auscultation (listening with a phonendoscope), characteristic noises are heard due to the turbulence created by blood as it flows into the aneurysmal sac and flows out.
The following instrumental research methods are used:
- plain chest x-ray - x-rays reveal a tumor-like formation that is associated with the thoracic aorta;
- Doppler ultrasound – using ultrasound, the wall of the thoracic aorta is examined and its expansion is detected;
- Magnetic resonance imaging (MRI) - the goal is the same as Doppler ultrasound, but the information content is higher.
conclusions
Due to the peculiarities of anatomy and physiology, the aorta is the leading vessel of the human body. It provides blood supply to all tissues, and therefore any of its pathologies lead to extensive disturbances in the functioning of the entire organism. In recent years, the mortality rate from vascular pathologies has been decreasing due to the introduction of new minimally invasive surgical treatment techniques.
The following sources of information were used to prepare the material.
Often aortic aneurysms
They are asymptomatic for a long time, their signs can be detected accidentally during a physical examination or ultrasound examination. Clinical manifestations of thoracic aortic aneurysms are partly considered in the differential diagnosis of myocardial infarction. As for abdominal atherosclerotic aneurysms, in more than 90% of cases they arise below the renal arteries and extend to the aortic bifurcation.
Aortic aneurysm
(from Latin apeitupo - expanding) - this is a local or diffuse expansion of its lumen 2 times or more greater than the diameter of unchanged areas or the normal size of the aorta for a given sex and age. Aneurysms occur due to various reasons that reduce the strength and elasticity of its wall.
To the development of aortic aneurysm
can cause various non-infectious and infectious diseases. Typically, the development of an aneurysm occurs when these diseases are combined with any hemodynamic and pathomorphological predisposing factors.
Of great importance in the formation of aneurysms of the thoracoabdominal aorta
have congenital degenerative diseases of the aortic wall, media necrosis, which are often found in Marfan syndrome, Ertheim disease, Ehlers-Danlos disease. In some cases, injuries to the chest and abdomen may have additional significance (sometimes they have independent significance).
Much less common than aortic aneurysm
occur with syphilitic, giant cell, mycotic aortitis. However, the most common cause of aneurysms of the descending thoracic and thoracoabdominal aorta is an atherosclerotic process. In some cases, atherosclerosis of the aorta can be combined with congenital inferiority of connective tissue, with degenerative processes in the aortic wall.
Arterial hypertension, combined with the above diseases
, together with atherosclerosis, is one of the leading risk factors in the development of aortic aneurysm. Almost all patients with distal aortic dissection and most patients with proximal aortic dissection have a history of hypertension. In this case, the level of diastolic pressure is of great importance.
Its increase is more than 100 mm Hg. st
. may play a decisive role in the occurrence of aortic rupture. Arterial hypertension is one of the risk factors for the development of aneurysm and aortic dissection, especially in the presence of degenerative connective tissue diseases and atherosclerosis. A significant number of patients with acute proximal aortic dissection have a history of or at the time of examination high blood pressure.
Some patients have aortic dissection
leads to a sharp disruption of general hemodynamics with the development of severe shock, and sometimes to cardiac tamponade. According to many authors (M.I. Kertes et al., etc.), important risk factors for rupture of aortic aneurysm are the following symptoms: diastolic blood pressure above 100 mm Hg. Art., the anteroposterior size of the aorta is more than 5 cm, especially against the background of severe chronic obstructive pulmonary diseases. In the presence of arterial hypertension and the diameter of the proximal aorta is 6 cm or more, and the distal part is 7.2 cm, the risk of aortic dissection and rupture increases significantly. The most common cause of death in the first weeks after the occurrence of dissection in the proximal aorta is its rupture with bleeding into the pericardial cavity and the development of cardiac hemotamponade.
Approximate average normal sizes of various sections of the aorta (according to M.I. Kertes et al.)
Aortic aneurysm clinic
Clinical manifestations of aortic aneurysm
largely depend on the presence or absence of delamination. Dissection of the aortic wall occurs due to the destruction of the inner and middle membranes. As a result, blood penetrates through the resulting defect between the inner and middle or between the middle and outer membranes, peeling them off one after another. In this case, an intrawall accumulation of blood is formed, which communicates with the lumen of the vessel. Subsequent symptoms are largely determined by the extent of the dissection and the duration of the disease.
Differential diagnosis
Differential diagnosis of thoracic aortic aneurysm is most often carried out with such diseases as:
- neoplasms of the mediastinum (structures between both lungs) – benign and malignant;
- coronary heart disease – a pain syndrome that occurs due to oxygen deficiency in the myocardium against the background of pathology of the coronary vessels;
- pericardial cyst is a cavity formation with fluid inside.
Postoperative period
After undergoing thoracic aortic replacement surgery, you must follow all the advice of your doctor:
- Moderate physical activity (start with a walk, then move on to light physical exercise that does not cause pain).
- Dieting. First you need to adhere to diet No. 0, it is used during rehabilitation. Next is No. 10, which is prescribed to all patients with diseases of the cardiovascular system.
- Before the patient is discharged from the hospital, bed rest is required.
- After discharge (for a month), driving a car, lifting more than ten kilograms, and taking a bath are prohibited.
- You must take all prescribed medications strictly as directed by your doctor.
- Healthy lifestyle. Stop smoking and alcohol. Try to be less stressed. Bring your weight back to normal, eat right.
Be attentive to your health. If you notice the following symptoms: body temperature 38 °C or more, pain in the legs, back, operation site, discharge from the wound (in open surgery), immediately call an ambulance.
Treatment of thoracic aortic aneurysm
The only way to radically rid a patient of a thoracic aortic aneurysm is through surgery. But the operation is not always performed - if the operational risks exceed the risk of complications of the aneurysm, then dynamic observation with regular repeated instrumental examinations is recommended to identify changes in the aneurysm wall, if any.
Indications for surgical treatment are:
- aneurysms with a diameter of 3-3.5 cm or more;
- increasing enlargement of the aneurysm - even if it is small in size;
- deterioration of the patient's condition;
- development of complications.
The extent of the operation depends on the degree of damage to the wall of the thoracic aorta. If the aneurysm is small, then it is excised and plastic surgery of the thoracic aorta is performed. In case of a large aneurysm, it is impossible to perform repair using one’s own tissues, so prosthetics are performed using artificial implants.
Prognosis and complications
The long-term prognosis for patients with a thoracic aortic aneurysm depends on other medical problems, such as heart disease, high blood pressure, and diabetes. The size of the aneurysm is the main factor predicting its rupture. The survival rate for an aneurysm larger than 6 cm is 38-64% . Aneurysm rupture is the most common cause of death in patients who refuse surgery.
After rupture, the patient dies within 6 hours. Surgery significantly increases the survival rate.
Possible complications after surgery include:
- Stroke;
- Kidney damage;
- Infection;
- Heart attack;
- Arrhythmia;
- Paralysis;
- Death soon after surgery occurs in 5% of patients.
Complications from stenting also include damage to the blood vessels supplying the lower extremities, which will require another surgery.
Prevention
The main measures to prevent the acquired form of this disease are:
- prevention of injury to the thoracic aorta;
- gentle performance of various manipulations on it;
- use of high-quality material when performing operations on the thoracic aorta;
- prevention, diagnosis and treatment of inflammatory, metabolic and infectious pathologies that can provoke the development of the described disease.
Important
It is not possible to prevent the occurrence of a congenital type of thoracic aortic aneurysm, but if a woman is provided with normal conditions during pregnancy, the risk of a congenital disorder is reduced.
How is a dangerous pathology treated?
Features of disease therapy
Adequate treatment of seals in the aorta of the heart is prescribed on the basis of a comprehensive diagnosis and the identified causes of the pathology. May be shown:
- conservative treatment;
- surgical intervention;
- Complication prevention program.
If the pathological process is caused by natural aging of the body in an elderly patient, then drug therapy and a pathology prevention program may be prescribed.
Medicines are prescribed to stabilize blood pressure, aimed at combating atherosclerosis, normalizing metabolic processes and treating identified diseases that have caused the formation of compactions in the cardiac aorta.
Attention! A patient with this diagnosis must register with a cardiologist and undergo periodic preventive examinations.
To treat thickening of the aorta of the heart, surgical intervention is also indicated. Depending on the complexity of the process, plastic surgery and prosthetics are prescribed (you can find out how such an operation is performed by watching a video on the Internet resource). In the most severe cases, an organ transplant from a donor is performed.
The complication prevention program is based on:
- nutrition adjustments;
- complete cessation of all bad habits (smoking, drinking alcohol);
- prevention of nervous tension and stress;
- avoiding excessive physical activity;
- taking daily walks in the fresh air.
An addition to the program is the preventive treatment of aortic thickening with folk remedies, in which the main emphasis is on juice therapy, daily consumption of large amounts of vegetables and fruits, reducing foods containing cholesterol and animal fats, and avoiding smoked and fried foods.
Materials used in the article:
https://med88.ru/kardiologija/patologii-serdca/uplotnenie-aorty-serdca-chto-jeto-takoe/
https://infocardio.ru/zabolevaniya-sosudov/uplotnenie-aorty-chto-eto-takoe.html
https://www.colady.ru/prichiny-i-priznaki-obmoroka-pervaya-pomoshh-chto-delat-pri-obmoroke-i-chego-delat-ne-sleduet.html
Post Views: 344
Forecast
The prognosis for an aneurysm of any segment of the thoracic aorta is complex due to possible complications that can lead to death.
Kovtonyuk Oksana Vladimirovna, medical observer, surgeon, consultant doctor
just today
( 51 votes, average: 5.00 out of 5)
The danger of a heart attack suffered on the legs
Heart murmur in children over 3 years of age and adolescents: causes, diagnosis, treatment
Related Posts
Aneurysm of the sinuses of Valsalva
An aneurysm of the sinuses of Valsalva, characterized by protrusion of the wall of one of the sinuses (their names correspond to the leaflets of the aortic valve - left coronary, right coronary, non-coronary) into the adjacent cardiac chamber, is usually a congenital anomaly (for example, in Marfan syndrome), caused by a weakness in the connection of the aortic wall with fibrous ring of the valve, although it can be recorded with aortoarteritis or supravalvular aortic stenosis.
The main morphological form of aneurysm of the sinuses of Valsalva is isolated in combination with other defects (septal defect, patent ductus arteriosus, coarctation of the aorta, bicuspid aortic valve, etc.).
An echocardiographic sign of this pathology is a saccular protrusion of the sinus wall into one of the cavities of the heart: the right - into the right atrium or the outflow tract of the right ventricle, the left - into the left atrium, the non-coronary - into the right atrium or the outflow tract of the right ventricle.
When a sinus ruptures, an echocardiogram performed from a parasternal approach in a short-axis view at the level of the aorta visualizes both the interruption of the echo signal in the area of the aneurysmal sac (single or multiple), and signs of volume overload of that chamber, damage to the right coronary sinus, most rarely - left sinus.
During Dopplerography and color circulation, turbulent blood flow in the corresponding cavity is recorded.
It is noted that in children it is possible to detect dilatation of the sinuses of Valsalva, most often non-coronary, in which the dilation of the sinus does not reach the level of an aneurysm. Long-term observation of such patients indicates the possibility of the benign nature of this pathology and its spontaneous disappearance as the child grows.