The largest vessel in our body is the aorta. Like any other vessel, it is susceptible to the formation of an aneurysm. Most often, an aortic aneurysm, a pathological enlargement of its section, occurs in the abdominal region, hence the name “abdominal aortic aneurysm.”
This condition often does not cause symptoms and is diagnosed accidentally, when presenting for another reason. This disease is rare, however, such a complication as a rupture of an aneurysm is very dangerous, as it can lead to death.
Treatment technologies at the Innovative Vascular Center
Vascular surgeons at our clinic have significant experience in open operations for abdominal aortic aneurysms. They have performed more than 150 operations for this pathology with success in 95% of patients. The approach of our clinic is to thoroughly prepare a patient with an aneurysm to exclude pathology of the heart and carotid arteries, which may affect the outcome of the operation. To prevent renal complications, we use prolonged hemofiltration in the postoperative period. To reduce blood loss, hemodilution (blood dilution) and blood return equipment are used. In order to prevent complications in the postoperative period, we practice early getting patients out of bed and active rehabilitation. In recent years, we have been gradually moving away from open operations for aneurysms in favor of less traumatic endovascular endoprosthetics operations.
Why is an aneurysm dangerous?
An aortic aneurysm may not manifest itself in any way at the initial stages of development. Sometimes there may be pain that is quite tolerable. However, this is a ticking time bomb. The main dangers of an aneurysm:
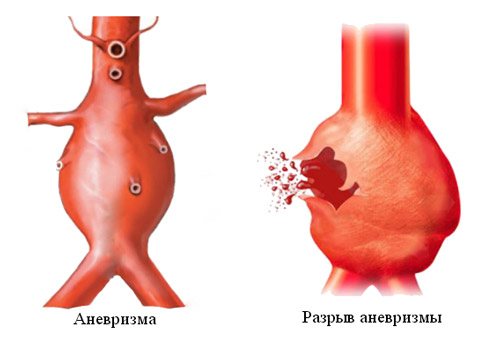
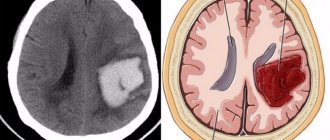
Break. Under certain conditions, the thinned wall of the aorta can rupture. This is a very serious complication. Without emergency surgery, a person dies from acute blood loss. Even an urgent blood transfusion will not help here (you cannot fill a leaky vessel).- Delamination. The wall of the aorta is multilayered; when one of the membranes is torn, the blood flow delaminates the wall. This process is accompanied by very severe pain, poor circulation, and shock.
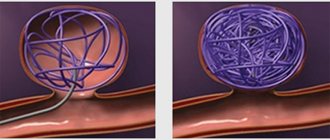
- Thrombosis in an aneurysm. In the area of protrusion of the aortic wall, turbulence in the blood flow occurs, and the speed of blood flow slows down here. Blood clots begin to form on the altered wall, gradually increasing in size. Blood clots are dangerous due to rupture and thromboembolism of the main and peripheral arteries.
- Pressure on neighboring organs. Depending on the location, a bulging and enlarged aorta can compress the organs of the mediastinum, bronchi, abdominal organs, and compress vascular bundles and nerve trunks.
Preparation for surgery for aortic aneurysm
- Before major aortic surgery, the patient should be examined in detail to reduce the risks of complications in other vascular territories. In our clinic, the treatment method for aortic aneurysm is determined by a council of doctors, taking into account the risks of the upcoming intervention.
- Electrocardiography and cardiac ultrasound are mandatory. To exclude postoperative bleeding from the stomach, esophagogastroscopy (EGD) is mandatory. A complex examination of the vessels of the heart, carotid arteries and arteries of the extremities is performed.
- On the eve of surgery, bowel preparation is performed. The patient does not eat dinner and takes special laxatives (fortrans). This achieves complete cleansing of the intestines and the risk of developing postoperative intestinal stagnation. A cleansing enema may be prescribed at night.
- On the morning of the operation, the abdomen, pubic area and thighs are carefully shaved. A catheter is inserted into the bladder and catheterization of the subclavian vein is performed. The patient is sedated and taken to the operating room.
Anesthesia during surgery
The operation can be performed under general anesthesia or under epidural anesthesia (injection in the back). General anesthesia is required for large aneurysms extending to the level of the renal arteries or higher. General anesthesia is required for access using a wide midline laparotomy. With retroperitoneal access to the aorta, epidural anesthesia can be limited. During operations for an aneurysm, cardiac activity and blood pressure must be monitored using special equipment. For anesthesia and intensive care, a catheter must be installed in the central vein (most often the subclavian). Kidney function is assessed by the amount of urine, for this purpose a catheter is inserted into the bladder. During anesthesia, the level of central venous pressure is monitored and drugs are administered to regulate the volume of circulating blood and electrolytes. If necessary, blood and plasma transfusions are performed to replace those lost during surgery. Special dispensers administer drugs that regulate blood pressure levels. During a long operation, a hemofiltration device may be connected to eliminate possible intoxication. Anesthesia during aortic surgery is very important and the comfort of surgeons and the immediate results of surgical intervention depend on its course.
Symptoms
A characteristic feature of an aneurysm is that for many years it can be completely asymptomatic . This is due to the rather slow growth of the aneurysmal defect . When the bag reaches a sufficient size, dull, aching and constant pain may appear, which will be localized mainly in the lumbosacral region and abdomen. Also, an aortic defect can be palpated in the form of a tumor-like formation, over which a systolic murmur can be heard. Characterized by decreased appetite, nausea and vomiting.
When an aneurysm ruptures, the patient feels sharp pain, a drop in blood pressure occurs, and tachycardia appears.
Progress of the aortic aneurysm resection operation
- Surgical approach
During the preoperative examination, a decision is made regarding the surgical approach. Most often, three accesses are performed. Two of them are in the groin area on the thigh, to isolate the common femoral arteries, one access is a median laparotomy (an incision in the middle of the abdomen) or an access on the left side. For tall aneurysms, the superior approach can be extended into the chest. This intervention is thoracophrenolumbotomy.
- The meaning of the operation
After isolating the aneurysmal sac, the abdominal aorta is clamped. The time for blocking blood flow must be reduced. To do this, before installing the clamp on the aorta, a good isolation of the aneurysm and all arterial branches up to the bifurcation of the aorta into the iliac arteries is performed. When vascular clamps are applied, the lumen of the aneurysm is opened, thrombotic clots are removed from the aneurysm cavity and bleeding from the branches flowing into the aneurysm is stopped.
Open intervention consists of replacing the enlarged section of the aorta with a synthetic vascular prosthesis. The latter is sewn into the upper section of the aorta (above the aneurysm), then the branches of the prosthesis are carried to the femoral arteries and sewn to them. After this, the prosthesis is covered with the walls of the aneurysmal sac. The main problem is the identification of the aneurysmal sac and the branches emanating from it. This must be done quickly enough if these branches are passable, since prolonged compression can cause disruption of the nutrition of the intestine or spinal cord.
After connecting the aorta to the femoral arteries, it is necessary to decide on the need for transplantation of the inferior mesenteric artery. This artery supplies blood to the colon, and sometimes ligating it can lead to disruption of the intestinal blood supply. To make a decision, it is necessary to evaluate the blood flow through this artery. If, after removing the clamp, there is good reverse blood flow, then the artery does not need to be sutured to the vascular prosthesis; if it is passable, but the blood flow is very weak, then the bypass paths are undeveloped and the arteries need to be replanted into the vascular prosthesis.
After completion of the vascular stage of the operation, tubular drains are installed in the retroperitoneal space and in the access area on the thighs, and the wounds are sutured layer by layer.
The average duration of surgery for an aortic aneurysm is 3 hours. The average volume of blood loss is about one liter. Blood loss is replenished with donor blood, plasma and saline solutions.
Risk factors
The disease is most common among men over 65 years of age, with aneurysm rupture occurring in 2 out of 50 cases, of which 1 is fatal .
Also at risk include:
- People who are overweight or obese;
- Patients who have already had cases of aneurysm or heart disease in their family;
- Patients with diabetes mellitus (especially type 2);
- Persons who experience persistently high blood pressure, aged 25 to 60 years;
- Patients with high levels of cholesterol and triglycerides in the blood;
- People leading a sedentary lifestyle;
- If the patient has abdominal injuries;
- Smoking greatly increases the possibility of developing and rupturing an aneurysm.
And:
- About one in 250 people over the age of 50 die from a ruptured aneurysm each year;
- This type of aneurysm affects 8% of people over the age of 65;
- Men are 4 times more likely to get the disease than women;
- Men over 60 who smoke and have atherosclerosis are most at risk;
- 50% of people die from a ruptured aneurysm because they do not seek professional help.
* according to the Society of Interventional Radiology - an American national organization of doctors.
Rupture of an abdominal aortic aneurysm during pregnancy is a rare but potentially fatal condition. Pregnant women are at risk. During pregnancy, many changes occur in the body that increase tension within the blood vessels, including the aorta. Pregnancy hormones have a direct effect on blood vessels. Some genetic diseases increase the likelihood of aneurysm rupture, for example, Marfan syndrome (an autosomal dominant hereditary disease characterized by connective tissue deficiency), Ehlers-Danlos syndrome (hereditary disease, hyperelasticity of the skin).
All women with aortic disease should be under constant supervision of specialists . The size of the aorta should be measured before conception (if an aneurysm has already occurred) and during pregnancy (against the background of conception there is a sharp increase in the aneurysm), it is very important that specialists exclude such possible complications as dissecting aortic aneurysm.
Taking into account the size of the aneurysm, experts assess the risk of surgical intervention before birth.
Complications during aortic surgery
Open surgery has a greater risk of early postoperative complications and mortality than endovascular aortic stent graft placement. Mortality after open surgery is about 5%, while after endoprosthetics it is 0.5%.
Other possible complications after resection of an aortic aneurysm:
- Acute renal failure
- Spinal cord stroke with leg paralysis
- High intermittent claudication (pain in the buttocks when walking) claudication
- Colon ischemia
- Embolism of the lower extremities with acute ischemia
- Bleeding from the surgical site and hemorrhagic shock
- Suppuration of the vascular prosthesis
These complications are quite rare. In our clinic, isolated cases of such complications were observed.
Prognosis after aortic replacement
The immediate postoperative period usually takes 10-14 days and depends on the immediate results of the operation. Within 1-3 days, patients require intensive care, and prolonged artificial ventilation is possible. We usually start lifting patients on the 3rd day after the intervention. We are allowed to walk by 5 days. If the postoperative period proceeds smoothly, the patient is discharged home on the 10th day.
After discharge, you must wear a special bandage on your stomach for a month. A month later, a control ultrasound scan is performed to assess the patency of the artificial prosthesis and the state of blood flow in the legs.
After open aortic surgery, the patient returns to normal daily activities after 3-6 months. The patency of vascular grafts is maintained at 93% over a five-year period after surgery. Ultrasound monitoring allows you to identify possible developments of problems and take timely measures to eliminate them.