In cardiology, pharmaceutical organic nitrates, whose more precise name is nitrovasodilators, are used to treat patients with angina pectoris, coronary artery disease, and acute coronary syndrome.

Short-acting nitrate is the best drug for self-relief of angina attacks
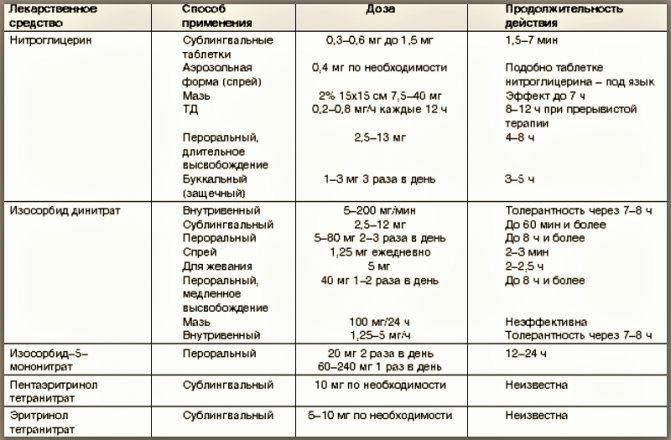
These heart medications today come in many forms: sublingual tablets, cheek patches, oral capsules, chewable lozenges, aerosols, sprays, ointments, skin patches, intravenous solutions.
The doctor decides which drug (active substance, duration of action, form) to prescribe to the patient. At the same time, he takes into account the diagnosis, stage of the disease, purpose of use, contraindications and side effects of nitrates.
How do drugs containing nitrates work?
The mechanism of action of nitrates is based on the fact that when they enter the body they are broken down into nitric oxide. Its molecules, through a chain of stimulation of a number of substances, ultimately increase the synthesis of cyclic guanosine monophosphate, which has a vasodilating effect on the endothelial cells of the cardiac chambers - relaxation of the vascular walls located in the smooth muscle tissue.

Ultimate vasodilating effects inherent in organic nitrates
You should know that this group of drugs expands the lumen of the venous vessels of the heart, both atherosclerotic and healthy. Moreover, in veins affected by atherosclerosis, this occurs only in those places where smooth muscle fibers are still preserved in the walls.
Where the narrowing occurred due to concentrically located plaques, expansion does not occur.
On a note. Medicines - blockers of b-adrenergic receptors and calcium channels, have less antianginal (coronary dilator) effect than nitrovasodilators.
In addition, the use of nitrates improves exercise tolerance. This occurs due to the fact that prolonged nitrovasodilators increase the threshold for the onset of ischemia of the heart muscle and improve the rheological properties of the blood, preventing platelet aggregation.
But the improvement in myocardial systolic function during treatment with nitrovasodilators occurs due to their anti-ischemic effect.
Indications for use
The main indication for the use of nitrates is vasospasm of the cardiac arteries, ischemia, and myocardial hypoxia. Relatively recently, medications were used for differential diagnostic purposes: with the help of Nitroglycerin, myocardial infarction was distinguished from angina pectoris (an attack of cardialgia was stopped by nitrates, a developing heart attack was not). Today, there are more accurate instrumental and laboratory methods for diagnosing AMI, but when providing first aid to heart patients, there is still no better alternative than Nitroglycerin or its analogues.
Nitrates are recommended for use when:
- myocardial ischemia of any origin (for the prevention of an attack of angina - before the planned exercise, for treatment - first aid);
- left ventricular failure;
- hypertensive crisis;
- acute heart failure (prevention or relief of pulmonary edema);
- CHF;
- arrhythmias due to deterioration of the trophism of the heart muscle;
- complex treatment or prevention of thrombosis, thrombophlebitis.
What about nitrates?
The modern classification of nitrates includes not only them, but also other drugs that have the same vasodilating effect:
- subgroup of sydnonimines - cormin, molsidomine, pirsidomine;
- other NO donors are amyl nitrite, Na nitroprusside.
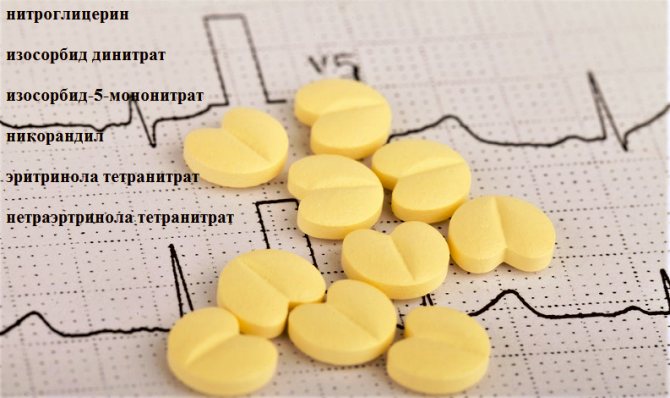
And the nitrate group includes medications, the active substances of which are listed in the photo.
Nitrates: list of drugs
Based on the duration of action, they are conventionally divided into:
- short-acting medications;
- moderately long-acting drugs;
- drugs with significantly prolonged action.
The first, including the fast-acting “classic of the genre” - nitroglycerin, act for up to 60 minutes, and the second, for example, molsidomine retard, from 1 to 6 hours.
Attention! Organic nitrovasodilators are characterized by significant variability in exposure. Only a doctor should prescribe the drug. The instructions included with the medicine will not help with self-medication. One patient will need a dose of 5 mg, another will need 100 mg.
But what drugs are classified as long-acting nitrates? The list of their active ingredients, which act from 6 to 16 hours, is headed by retard tablets of isosorbide dinitrate and isosorbide-5-mononitrate.
In fact, if a quick effect is needed, then sublingual (sublingual) forms of drugs are used; for moderate-long-term action, cheek stickers, lozenges, aerosols and sprays are suitable, and for prolonged action - ointments, skin patches, retard tablets or capsules.
Classification of nitrates
Over time, Nitroglycerin ceased to be the only representative in the presented group of antianginal drugs. Many analogues have appeared, as well as medicines with a similar structure, but in a more convenient form. All this necessitated the creation of a classification of nitrates.
There are several subgroups. The classification criterion is the main active substance. In the treatment of coronary heart disease, and in particular angina, 4 out of 5 subgroups are used.
Preparations based on Nitroglycerin
Medicines from the nitroglycerin-based group include:
- actual tableted Nitroglycerin, produced in glass bottles
- Nitrolingval spray for sublingual use
These are short-acting nitrates.
To treat manifestations of ischemia, intravenous analogues of Nitroglycerin are used. These include Nitropol. Bottles with Nitrostat and Perlinganite are also produced.
Long-acting representatives of this subgroup are in particular demand. Popular products include Nitro in the form of ointments, Nitrong, Trinitrolong, and Sustak.
Products with isosorbide mono- and dinitrate
In addition to drugs based on Nitroglycerin, there are products with isosorbide mononitrate, for example, Efox
Isosorbide mono- and dinitrate is considered a good alternative to nitroglycerin and its analogues. Among the drugs based on these active ingredients, short-acting and long-term drugs are also produced.
Reception features
In patients with stable angina (I–II), nitrovasodilators should be taken intermittently, namely immediately before situations that can cause a heart attack. Forms of short and moderately prolonged duration are suitable for this.
Treatment and relief of angina attacks with nitrovasodilator drugs
For angina pectoris (III–IV), either medications are prescribed with a regular duration, but 3–4 times a day, or prolonged forms, for example, isosorbide dinitrate retard, but 1–2 times a day and so as to ensure a therapeutic effect in during the day.
On a note. You should strictly follow the doctor's prescriptions and instructions - withstand short-term withdrawal, take intermittent doses, and do not give up other medications. This will help reduce the formation of tolerance to the nitrovasodilator, as well as withdrawal syndrome.
By the way, those taking ACE inhibitors with the active ingredients enalapril and perindopril should be aware that they potentiate (strengthen) the effect of organic nitrovasodilators.
Modern aspects of the use of nitrates in cardiology
Belarusian Research Institute of Cardiology
Nitrates are the most well-known group of drugs, maintaining their leading position in cardiological practice for over 100 years. In addition, every year new, previously unknown effects of their action are discovered, new representatives of this class of compounds are synthesized, and schemes for their application and areas of use are improved. Nitrates open the list of main antianginal drugs.
Currently, the group of nitrates is represented by three main organic compounds: glycerol trinitrate - niggroglycerin, isosorbide dinitrate and its “daughter” form - a mononitrate metabolite - isosorbide-5-mononitrate. Other organic nitrates, such as erinyl tetranitrate, pentaerythrol tetranitrate (erinitrate), due to their low effectiveness in the doses in which they are currently produced, have not yet received widespread use.
Organic nitrates, and these are the ones we will talk about, are polyol esters of nitric acid. Nitroglycerin was first synthesized by Sobrero in 1846 as an oily liquid. The history of its use in angina begins in 1879, when Dr. Murrell in the Lancet published the results of a study of the effect of nitroglycerin, first on himself and then among patients with angina in the form of a 1% alcohol solution.
In 1925, capsules with nitroglycerin were introduced into practice, then a liquid alcohol solution and tablets for sublingual use.
At the end of the 60s. Long-acting forms of nitroglycerin appeared in the 70s. - ointment with nitroglycerin, and later with isosorbide dinitrate.
At the end of the 70s. they began to use nitroglycerin solutions for intravenous administration, and in 1979 in the USSR a fundamentally new dosage form was created in the form of copolymer plates - trinitrolong.
In 1981-1982 The first transdermal forms of nitrates began to be used, and in 1983, aerosol forms for the relief of angina attacks.
Progress in the development of dosage forms of organic nitrates was due to the need to find more advanced drugs for the treatment of coronary artery disease and the desire to “bypass” the liver barrier, where nitroglycerin is metabolized by 60-80%. Then its effect is realized through metabolites, in particular mononitrates. Interestingly, none of the forms has lost its importance to this day, and now cardiologists use all six forms of nitrates, namely: tablets (or granules) for sublingual administration, tablets for oral administration (usually long-acting), infusion form nitroglycerin specifically for intravenous administration, buccal plates (or tablets), aerosol and transedermal (patches and discs) forms. These forms include preparations of both nitroglycerin and isosorbide dinitrate.
The main mechanism of action of nitrates is vasodilation. They are also called direct dilators, since they cause relaxation of the smooth muscle cells of veins and arteries directly, and not through the neuroendocrine system. Their action is similar to the endothelium relaxing factor, discovered and studied in the last 10 years. Chemically, it is nitric oxide, which is formed from L-arginine, relaxes vascular smooth muscle cells through activation of guanyl cyclase and acts only locally, providing, in addition to relaxation, inhibition of platelet aggregation and adhesion. In the case of atherosclerosis, they try to explain the vascular spasm by the absence of this factor in the vascular wall. The biological effect of nitric oxide ends after its oxidation into NO2 and NO3. The half-life of nitric oxide is 3-5 seconds.
Nitroglycerin and other organic nitrates cause vascular relaxation, independent of the above mechanism, after entering the smooth muscle cell, where they are converted into inorganic nitrates and nitric oxide. This conversion reaction requires the presence of sulfhydryl groups, which are nitrate receptors on cell membranes. Subsequently, nitric oxide triggers the same mechanism: activation of guanyl cyclase - the formation of cyclic guanosine monophosphate. The latter causes relaxation of smooth muscles by accelerating the release of Ca ++ from cells.
Consequently, nitric oxide is a substance that combines an endogenous factor and a factor formed from the metabolism of exogenous nitrates.
As a result of relaxation of blood vessels, mainly venous ones, the following effects occur:
1) expansion of peripheral veins leads to a decrease in venous blood flow and, as a consequence, to a decrease in end-diastolic pressure and ventricular volume, i.e. cardiac preload decreases. As a result, the tension of the ventricular wall decreases, the filling pressure of the subendocardial coronary vessels increases and coronary circulation improves;
2) dilatation of peripheral arteries leads to a decrease in peripheral resistance and a decrease in cardiac afterload;
3) large coronary vessels dilate, collateral circulation increases and oxygen supply to ischemic areas of the heart muscle improves.
The overall effect (due to a decrease in pre- and afterload) is expressed in a decrease in the oxygen demand of the heart muscle and an impact on the main pathogenetic mechanism of IHD.
The listed effects of nitrates make it possible to use them not only for coronary artery disease (angina), but also for the treatment of heart failure, especially in the early stages of its development. However, there is evidence that in patients with severe circulatory failure, significantly increased pressure in the right atrium and peripheral edema, nitrates often do not have a good effect.
Nitrates have also found use in the treatment of pulmonary hypertension, especially in acute conditions. At the same time, there is no clear opinion about their suitability for long-term treatment of pulmonary hypertension. It is noted that with long-term treatment the effect gradually decreases, and this, according to many researchers, is mainly due to the development of tolerance to the effects of nitrates.
Characteristics of dosage forms of nitroglycerin. Tablets, capsules and inhalation forms for sublingual administration are short-acting nitroglycerin preparations and are used only for the relief of angina attacks. When using nitroglycerin granules, especially domestically produced ones, one should be aware of the rapid (after 60-70 days) loss of their effectiveness in opened bottles. Patients are advised to periodically change tubes of nitroglycerin or have a spare unopened one.
Aerosol preparations (isomak spray, isoket, nitromint, etc.) do not have any special advantages over sublingual tablets, and their distribution is currently limited due to the content of freon in the cans as an environmentally harmful substance. The effect of nitroglycerin occurs within 1-2 minutes and reaches a maximum after 4-6 minutes. After 20-30 minutes, nitroglycerin is no longer detectable in the blood, therefore, if there is no relief effect after the first tablet, repeated administration is recommended after 3-5 minutes.
Infusion forms are currently the main treatment for patients with acute myocardial infarction and unstable angina. Intravenous infusion is usually started at a rate of 5-25 mcg/min and then the dose is titrated, increasing the rate of administration until the systolic pressure decreases by 10-20% (but not lower than 90 mmHg) or the pulmonary capillary wedge pressure by 20-30%. The antianginal effect usually occurs quickly - after 2-5 minutes, but maintenance infusion in patients with acute infarction is usually carried out for approximately 10 hours. The most well-known drugs are perlinganite (a concentrated aqueous solution of nitroglycerin in an ampoule of 10 mg in 10 ml of solution or in a bottle of 50 mg in 50 ml of solution) and isoket. Before intravenous administration, it is dissolved in an isotonic sodium chloride solution or in a glucose solution. Vials with nitroglycerin solutions should be protected from light.
Tablets for oral administration (oral) - long-acting drugs - are manufactured in such a way that part of the nitroglycerin is quickly absorbed in the gastrointestinal tract and begins to act after 10 minutes, and part is absorbed more slowly and provides an effect within 4-6 hours. They are intended only for ( !) to prevent, but not relieve, attacks of angina. As a rule, they are available in two dosages - mita and forte (trinitrates), simple and retard (dinitrate and mononitrate). The dosage of simple forms is 2.5-20 mg, and tablets containing 2.5-10 mg of isosorbide dinitrate can be used for sublingual administration. Extended-release tablets (retarded) are available in doses of 20, 40, 60 and 120 mg. All available preparations of nitroglycerin, isosorbide dinitrate, isosorbide-5-mononitrate in sufficient dosages have approximately the same antianginal effectiveness. For trinitrates (nitroglycerin), a single dose should be at least 6.5 mg (the effect of these doses is no different from the placebo effect - this has been proven through special pharmacodynamic studies). During the first passage through the liver, the forms are almost completely destroyed. Single doses of isosorbide dinitrate and isosorbide-5-mononitrate are 10-30 mg. The advantage of mononitrates is that they are little destroyed in the liver and tolerance practically does not develop to them (monomak, monicor, pentacard, opicard, imdur, etc.). Retard forms can be taken once a day. The frequency of administration of simple forms is determined by the severity of angina pectoris: the higher the functional class of coronary insufficiency, the more frequently they should be used.
There are also combined preparations from the nitrate group, for example nitrodurate (Germany), containing 0.5 mg glycerol trinitrate + 5 mg isosorbide dinitrate.
The maximum effect of nitrates when taken orally begins after 60-90 minutes.
Buccal plates or tablets for application to the mucous membrane of the upper gum are available in doses of 1, 2 and 4 mg; they are able to stop an attack of angina in the same time frame as tablets for sublingual administration, and prevent it within 3-5 hours. They have high bioavailability . Domestic drugs are trinitrolong and dinitrosorbilong. The latter is available in 40 mg tablets and provides a duration of action of more than 10 hours. Imported drugs of a similar form: susadrin, sustabukal, nitrobucal (Yugoslavia), nitrogard, suscard.
Transdermal forms (patches, discs, ointments) are used to prevent angina attacks. Duration of action is 12-24 hours, onset of action is after 30-60 minutes. This dosage form has already passed the peak of its incredible popularity. Its disadvantages are unstable bioavailability, local irritation, high cost, lack of a stable effect throughout the day and the ability to cause not only tolerance, but also tachyphylaxis (rapid addiction) to nitrates. Proprietary names: nitro-derm, nitro-lor, minitron, nitrodur, diafusor, nitro ointment, etc.
Nitrates are the drugs of choice for patients whose anginal syndrome is quickly relieved by sublingual nitroglycerin, when angina is combined with circulatory failure, pulmonary hypertension, or with initial bradycardia. It must be taken into account that with an increase in the dose of nitrates, the duration of their action significantly increases.
An important point in treatment with nitrates is the recently discovered fact of a decrease in the antianginal effectiveness of nitrates with long-term use due to the development of tolerance to nitroglycerin, i.e. a condition in which a constant increase in the dose of the drug is required to achieve the same antianginal or hemodynamic effect.
Most often, tolerance develops to transdermal forms of nitrates. It is believed that the development of tolerance is caused by the occurrence of a deficiency of sulfhydryl groups and a change in the synthesis of CGMP, therefore, to eliminate or weaken the severity of tolerance to nitrates, it is proposed to use donors of sulfhydryl groups, for example, unithiol, methionine, dibunol and even capoten. There is also an opinion that the weakening of the effect of nitrates is observed due to a systemic drop in blood pressure, in response to which a neurohumoral reaction occurs: the tone of the sympathetic nervous system increases and the synthesis of renin-aldosterone increases, followed by water retention. This leads to a return of the filling pressure of the left and right ventricles to initial or higher values. In this regard, every 1.5-2 months of course intake of nitrates, it is necessary to take a break for 1-2 weeks. During this time, the effectiveness of nitrates is restored. If it is not possible to completely cancel nitrates, then Corvaton (Sidnopharm) or Corinfar can be prescribed during the break.
For the same reason, it is justified to take nitrates before upcoming physical activity or before expected attacks of angina pectoris - the so-called intermittent regimens of nitrates, in which there are intervals during the day free from the action of the drugs (8-12 hours or more).
It should be taken into account that the time of appearance and severity of the weakening of the effect of nitrates are not the same for each patient and different vascular zones. According to our data, the effect of nitrates decreases most quickly on the pulmonary circulation, then on the volumes of the ventricles, and lastly on the peripheral arterial vessels and coronary circulation, therefore, when assessing the development of tolerance, it is necessary to use complex data. To prevent tolerance, you can change the route of administration of nitrates into the body, using different dosage forms, for example, replace oral administration with sublingual, trinitrates with dinitrates, and even better, mononitrates.
Contraindications: hypersensitivity to nitrates (severe headache, hypotension, tachycardia), acute cerebrovascular accident, increased intracranial pressure, state of shock or collapse, acute myocardial infarction occurring with hypotension, collapse. Caution is necessary in case of severe cerebral atherosclerosis and pregnancy.
In conclusion, it should be noted that the indications for the use of nitrates will certainly expand in the future, and drugs from this group will be successfully used in the treatment of many diseases of the cardiovascular system.
Medical news. – 1995. – No. 3. – P. 2-7.
Attention! The article is addressed to medical specialists. Reprinting this article or its fragments on the Internet without a hyperlink to the source is considered a violation of copyright.
Indications for taking nitrates. Side effects of nitrates.
Indications for taking nitrates
. periodic attacks of HS, low effectiveness of AB or BMCC, patients with hypertension, low exercise function and obvious CHF. In patients with TS, but without symptoms or BMI, or concomitant LV failure, the administration of nitrates is not indicated. Fast onset nitrates
• cerebral symptoms (the most common) - a sharp headache, a feeling of “fullness” and pulsation of the head, dizziness, noise in the ears and head are not grounds for replacing nitroglycerin with less effective drugs. These sensations are short-term (often pass or weaken within a few days), do not threaten the patient’s life, you just need (and can!) get used to them. Such effects are reduced by the combination of nitroglycerin with validol (menthol), caffeine preparations or venotonic drugs. Still, up to a third of patients cannot use nitrates because of headaches;
• palpitations caused by reflex sinus tachycardia (it is corrected with AB);
• nausea, vomiting;
• episodes of skin redness;

• orthostatic hypotension - a decrease in blood pressure by more than 15 mm Hg. Art. from the initial level (with intravenous administration of large doses of nitrates, which also act on the arterial bed). It can be reduced by changing body position. Often the cause of a drop in blood pressure is a combination of nitrates with ACE inhibitors and BMCC;
• “withdrawal syndrome” (with a sudden cessation of their intake into the body) in the form of exacerbation of coronary insufficiency and increased blood pressure;
• rapid addiction (tachyphylaxis) and the emergence of tolerance (decreased sensitivity) to nitrates, developing with standard use (1 tablet 3 times a day) of a long-acting drug. Tolerance to nitrates depends on the dose and may appear 24 hours after the start of treatment. Therefore, to obtain an adequate effect, the patient must gradually increase the dose and frequency of taking the drug.
The basis of the phenomenon of nitrate tolerance
lie: the appearance of a deficiency of intracellular SH groups (necessary for the appearance of N0); neurohormonal activation (renin-angiotensin system with subsequent increased release of catecholamines into the bloodstream); restructuring of nitrate receptors; increased production of free radicals that destroy NO. They should be used in minimally effective doses during periods of deterioration (except for patients with severe TS); replace oral forms of nitrates with intravenous ones when this phenomenon occurs or alternate with other anti-ischemic drugs. It is more correct to prescribe nitrates before the supposed additional physical activity that causes attacks of TS (treatment “as needed”, the peak drug concentration should coincide with the maximum physical activity). So, if a patient goes to work at 8 a.m., then nitrates should be taken 1 hour before the expected load (i.e., at 7 a.m.).
Sensitivity to nitrates
is restored after a certain period free from taking them. Therefore, in order to avoid tachyphylaxis, treatment with them should be intermittent - the duration of the “nitrate break” should be sufficient, at least 8 hours during the day (if the nitrate-free period exceeds 8-12 hours, then tolerance to them usually does not develop). An alternative is molsidomine therapy (it differs from nitrates in chemical structure, but nothing in its mechanism of action).
For stable angina
FC3 prescribe long-acting nitrates.
Contraindications to taking nitrates
. allergic reactions to them; ALV with low LV EDD; RV MI; increased intracranial pressure; acute cerebrovascular accident (ACVA), stroke; low SBP less than 100 mm Hg. Art. or DBP less than 60 mm Hg. Art.; severe stenosis of the aortic and mitral heart valves.
Contents of the topic “Treatment of angina pectoris. Algorithms for the treatment of angina pectoris.":
►Ecotester. How to reliably determine the amount of nitrates in a product in 20 seconds? (SOEKS Ecotester)
Contraindications
Nitrate intake is limited in many cases. First of all, these are common pathological conditions that require emergency intervention and pose a risk to life. For example:
- vascular collapse with a drop in blood pressure below 90 mm Hg. Art.;
- cardiogenic shock;
- a sharp drop in blood pressure;
- attack of myocardial ischemia;
- head injury;
- high intracranial pressure;
- ONMK;
- angle-closure glaucoma;
- anemia;
- pulmonary edema;
- uncontrolled arrhythmia:
- hypersensitivity to drugs.
Nitrates are recommended with caution to patients diagnosed with cerebral atherosclerosis. During pregnancy, drugs in this group can cause intrauterine fetal death. Breastfeeding involves giving up nitrates or transferring the baby to artificial formulas, since, when penetrating into breast milk, the drugs cause hemodynamic disorders in the baby, methemoglobinemia.
Side effects
Side effects when using nitrates are also not uncommon. They can be conditionally divided into two groups: frequently occurring and observed in exceptional cases. The first group includes:
- vascular pulsations, migraine;
- hypotension, VSD;
- orthostatic collapse;
- cardiopalmus;
- slowing of the pulse during intravenous infusions;
- redness of the face;
- rapid addiction to drugs;
- withdrawal syndrome;
- symptoms of intoxication;
- retrosternal discomfort;
- hypoxia with cyanosis of the nasolabial triangle (life-threatening).
Rare side effects from taking nitrates include:
- high intraocular pressure;
- skin rashes;
- dyspepsia;
- methemoglobinemia.
Medications
Medical substances close to organic nitrates (sodium nitroprusside, nitrites, molsidomine) also have a nitroxidergic effect.
They have well-known differences in pharmacokinetic parameters and indications for use (nitroglycerin is used mainly to eliminate angina attacks, other medications are used to prevent their development). Adverse reactions of individual medications are mainly due to the mechanism of action common to the entire category of these drugs, and therefore are very similar.