Main clinical symptoms
Unstable angina (indicating Braunwald class)
- The transition of angina to a higher FC, up to angina at rest, or angina at rest becomes more severe or attacks of angina occur for the first time in the previous month.
- Pain syndrome or its equivalents, unusual (for a given patient) severity and duration, expansion of areas of pain irradiation, decreased effect of nitrates, increased frequency of attacks;
- ECG: changes in the final part of the ventricular complex are possible.
Acute coronary syndrome (ACS)
- For arterial hypertension: stage I-II-III hypertension. AH I-II-III degree. Complicated hypertensive crisis. Acute coronary syndrome
- With normal blood pressure levels: coronary artery disease. Acute coronary syndrome
Intermediate diagnosis during initial contact with the patient, when it is clinically difficult to differentiate unstable angina and myocardial infarction.
ECG:
- Option 1 – ACS without ST elevation
- Option 2 – ACS with ST elevation.
Classification of angina pectoris
FC I The person tolerates normal load well. Attacks of angina occur only under significant loads. FC II. Physical activity is limited. Seizures occur when walking more than 500 m, when climbing stairs more than one floor. The likelihood of angina attacks increases when walking in cold weather, against the wind, during emotional excitement, or in the first hours after waking up. FC III. Marked limitation of usual physical activity. Seizures occur during normal walking on level ground at a distance of 100-500 m, or when climbing stairs to one floor. FC IV. Angina pectoris occurs with light physical exertion, when walking on level ground for a distance of less than 100 m, and also at rest. Stopping the exercise and taking nitroglycerin for angina pectoris usually stops the pain attack!
Diagnostic measures
Unstable angina
- Taking anamnesis (simultaneously with diagnostic and therapeutic measures);
- Examination by an emergency medical technician (paramedic) or a medical specialist from a visiting emergency medical team of the appropriate profile;
- Registration of an electrocardiogram, decoding, description and interpretation of electrocardiographic data;
- If clinical manifestations of the disease last > 2 hours:
- Express examination of troponin levels in the blood;
- Pulse oximetry;
- General thermometry.
Acute coronary syndrome
- Scope of diagnostic measures according to the “Acute myocardial infarction” protocol.
Diagnostics
Often, an experienced cardiologist can make a diagnosis of angina based on complaints and a detailed collection of family and household history. To confirm the diagnosis, a number of instrumental research methods are required. ECG is a simple, accessible and informative method for diagnosing angina pectoris. The most informative is the ECG, which is taken during a painful attack. A special role in the diagnosis of angina pectoris is given to stress tests (bicycle ergometry, treadmill test, cold test, etc.), as well as ECG monitoring (Holter monitoring). During stress tests, conditions are created that increase the myocardial oxygen demand, which makes it possible to identify possible myocardial ischemia during exercise. Holter monitoring involves monitoring an ECG recording with a special portable device for a whole day. In this case, the patient keeps a diary where he records the load. Analysis of these data also makes it possible to identify episodes of myocardial ischemia. Ultrasound of the heart. It is performed to assess the condition of the valve apparatus and identify disturbances in myocardial contractility, which can serve as an indirect sign of myocardial ischemia. Data from a biochemical blood test (cholesterol, lipid profile, etc.) may indicate an increased risk of atherosclerotic vascular damage. Myocardial scintigraphy is a non-invasive method that allows you to get a fairly clear picture of damage to the coronary arteries. The method is not widely used due to its high cost. Coronary angiography is an invasive x-ray examination of the coronary arteries. Gold standard for diagnosing coronary heart disease. The method allows you to obtain a detailed understanding of the nature of damage to the arteries of the heart. Indications for coronary angiography are set by a cardiologist based on previous research methods.
Therapeutic measures
Unstable angina
- Providing a medical and protective regime;
- Horizontal position;
- Nitroglycerin – 1 tablet sublingually or
- Nitroglycerin (spray) – 1 dose sublingually;
- Inhalation administration of 100% O2 at a constant flow through a mask (nasal catheters);
- If pain or its equivalent after 3 minutes:
- Nitroglycerin – 1 tablet sublingually or
- Nitroglycerin (spray) – 1 dose sublingually;
- Catheterization of the cubital or other peripheral veins;
- If pain or its equivalent persists:
- Morphine - IV slowly in fractional doses of 2-3 mg every 2-3 minutes until the effect occurs or up to a total dose of 20 mg;
- Metoprolol – 25 mg orally or 5 mg IV bolus slowly at a rate of 1 mg/min. or
- Anaprilin – 10 mg orally;
- Aspirin – 250 mg (crushed) sublingually;
- Heparin – 60-70 units/kg IV bolus (maximum 5000 units) or
- Fondaparinux (Arixtra) – 2.5 mg IV bolus or
For patients under 75 years of age:
- Enoxaparin (Clexane) – 30 mg IV bolus, h/w 15 minutes 1 mg/kg (not more than 100 mg) subcutaneously;
Patients 75 years of age and older:
- Enoxaparin (Clexane) – 0.75 mg (not more than 75 mg) subcutaneously;
- For patients under 75 years of age:
- Clopidogrel – 300 mg orally;
Patients 75 years of age and older:
- Clopidogrel – 75 mg orally;
- If pain or its equivalent persists:
- Nitroglycerin (Isoket, Perlinganite) – 10 mg IV drip, at a rate of 10 mcg/min, increasing the rate of administration by 5-10 mcg/min every 10 minutes. up to 200 mcg/min., under the control of blood pressure and heart rate, on site and during medical evacuation;
- For arterial hypertension :
- Nitroglycerin (Isoket, Perlinganite) – 10 mg IV drip, at a rate of 10 mcg/min, increasing the rate of administration by 5-10 mcg/min every 10 minutes. up to 200 mcg/min., under the control of blood pressure and heart rate, on site and during medical evacuation or
- Clonidine (Clonidine) – 0.05-0.1 mg IV bolus slowly;
- Medical evacuation (see “General tactical measures”).
Acute coronary syndrome
- Scope of treatment measures according to the protocol “Acute myocardial infarction”
What is unstable angina?
Pathology is a period of IHD - coronary heart disease.
Unstable angina is called the borderline stage between myocardial infarction and simple deterioration of blood circulation.
The disease code according to ICD-10 is I20.0. Differences between this form of angina and stable angina:
- unpredictability of the conditions for the occurrence of attacks;
- rapid development of the disease;
- low effectiveness of Nitroglycerin during an attack;
- high risk of developing a heart attack.
Conditions of occurrence
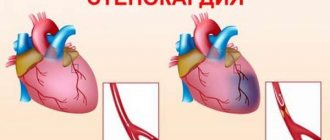
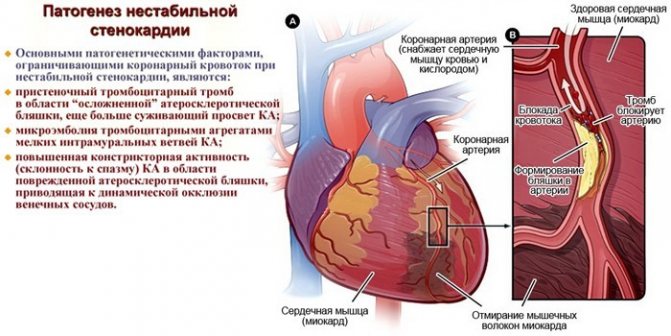
Unstable angina is caused by narrowing of the lumen of the coronary arteries. When it decreases by 50%, blood flows poorly to the heart and ischemia develops. The myocardium experiences a lack of oxygen, metabolic products are not excreted, and pain occurs behind the sternum.
In an unstable form of pathology, an attack develops with a sharp disruption of blood circulation in the coronary arteries.
This occurs against the background of atherosclerosis according to the following mechanism:
- Large plaques rupture and platelets accumulate on their surface.
- A blood clot appears - a thrombus, which more closely blocks the lumen of the artery.
- A spasm of the vessel occurs, the blood flow to the heart suddenly stops.
Danger to life
Unstable exacerbations with the development of coronary artery disease have a high risk of necrosis of the heart muscle and sudden death of the patient. About 80% of heart attacks with this history occur in the first week. Other dangerous complications of pathology:
- chronic heart failure;
- pulmonary edema;
- arrhythmia – heart rhythm disturbances;
- tachycardia.
General tactical measures
Unstable angina
For teams of all profiles, except cardiology and intensive care:
- Provide therapy;
- When stopping an anginal attack, stable hemodynamics, electrical stability of the myocardium, the ambulance transport is equipped with medical equipment necessary to provide assistance to cardiac patients, consultation with a doctor at the Central Clinical Hospital:
- Perform medical evacuation.
In other cases:
- Call the cardiology (resuscitation) team;
- Carry out therapy before transferring the patient to the cardiology (resuscitation) team.
For cardiology and resuscitation teams:
- Provide therapy;
- Perform medical evacuation.
Treatment of unstable angina
The goal of therapy is to prevent myocardial infarction.
Treatment is carried out in a hospital, tactics are chosen based on ECG results.
The patient is prescribed bed rest. Directions of therapy:
- eliminate cardialgia;
- get rid of the underlying disease.
Treatment of all forms of angina with an unstable course is complex, the following methods are used:
- use of medications - injections, infusions, tablets before and after surgery;
- surgical intervention - in case of a variant form of the disease, the development of severe complications;
- diet therapy - reduces the risk of a recurrent attack, improves the condition of blood vessels and blood flow.
Article on the topic: Urine for diastasis - how to take it and interpretation of the results, normal indicators for children and adults
Medication
As a pain reliever during an attack of angina, the patient is given Nitroglycerin under the tongue and administered through a dropper with Heparin. Afterwards, to treat an unstable form of pathology in order to eliminate its symptoms, the following drugs are used:
- Anticoagulants (Heparin) - inhibit blood clotting and thin it, preventing the formation of blood clots. Administration intravenous and subcutaneous.
- Lipid-lowering drugs (Atorvastatin) - normalize cholesterol levels in patients with atherosclerosis. Used in tablets, they reduce the risk of new attacks of angina.
- Disaggregants (Clopidogrel, Aspirin) – prevent platelets from sticking together.
- Calcium channel antagonists (Verapamil) - reduce myocardial oxygen demand, dilate blood vessels and improve blood supply to the heart.
- Diuretics (Furosemide) - eliminate swelling, remove excess fluid, are indicated for heart failure.
- ACE inhibitors (Enalapril) - block the synthesis of an enzyme that constricts blood vessels, reducing blood pressure.
- Beta-blockers (Anaprilin) - reduce the strength and frequency of heart contractions, are prohibited for Prinzmetal's angina.
Surgical
In case of a large area of ischemia, rapid progression of pathology, heart failure and damage to large arteries, an operation is indicated, which is performed using the following methods:
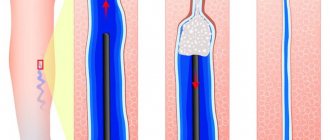
- Angioplasty is a minimally invasive treatment in which the doctor inflates the lumen of a narrowed vessel using a catheter with a balloon. The operation is performed through a puncture of the femoral artery with local anesthesia. Symptoms of the pathology disappear completely in 60% of patients.
- Coronary artery bypass grafting is performed when the main artery stenosis is above 50%. The doctor creates a bypass for blood flow through a shunt, which is attached below the area of narrowing of the lumen and to the aorta. The condition improves in 80% of patients, angina resolves in 63%. The risk of heart attack after such an operation is 7%.
- Intracoronary prosthetics or stenting - a conductor is inserted into the area of narrowing of the artery and a balloon catheter is placed. He inflates the vessel and the doctor places a stent in the area of stenosis: a tube made of metal fibers. The design expands the gap and prevents the walls from sticking together. The stent is drug-coated, which reduces the risk of new stenosis. The disadvantage of this design is that it slowly “grows together” with the wall of the vessel.
catalogue of articles
Modern methods of treatment of coronary artery disease, angina pectoris Standards for the treatment of coronary heart disease, angina pectoris Protocols for the treatment of coronary artery disease, angina pectoris CHD
, angina pectoris
Profile:
therapeutic.
Stage of treatment:
outpatient.
Purpose of the stage:
1. selection of therapy; 2. improvement of the general condition of the patient; 3. reduction in the frequency of attacks; 4. increasing tolerance to physical activity; 5. reduction of signs of circulatory failure.
ICD10 code:
I20.8 Other forms of angina.
Definition:
Angina is a clinical syndrome manifested by a feeling of tightness and pain in the chest of a squeezing, pressing nature, which is most often localized behind the sternum and can radiate to the left arm, neck, lower jaw, and epigastrium. The pain is provoked by physical activity, going out into the cold, eating a large meal, emotional stress, goes away with rest, and is eliminated by nitroglycerin within a few seconds or minutes.