Quite often we are negligent about our health, which sometimes leads to the worst turn of events. In the absence of proper and timely treatment, there is always a high risk of subsequent complications. One of these complications may be a disease called cerebral arachnoiditis, which accounts for 3 to 5 percent of diseases of the nervous system. The course of the disease and its consequences can be different, ranging from mild, if treatment was prescribed immediately, to the death of the patient.
Causes
Arachnoiditis is considered a serious disease that occurs in childhood and in people under 40 years of age. In 10-15% of cases, arachnoiditis has unknown causes. In other situations, the cause of arachnoiditis is a consequence of past illnesses:
- Acute and chronic infectious diseases - viral infections such as influenza, measles and viral meningitis. Purulent lesions in the sinuses, otitis media, inflammatory processes in the mouth, ARVI and other diseases.
- Traumatic brain injuries - brain contusion or subarachnoid hemorrhage.
- Other causes may also include inflammation due to slow-growing tumors and encephalitis.
- Influenza is most often identified as the main cause.
People with chronic fatigue and overwork, alcohol and other intoxications have a predisposition.
Pathogenesis of the disease
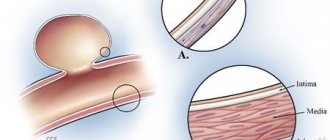
To understand what arachnoiditis is, it is necessary to understand the process of its development. Between the hard and soft membranes of the brain there is connective tissue that looks like a spider's web. It is separated from the soft shell by the subarachnoid space, in which cerebrospinal fluid circulates and blood vessels are located, the task of which is to nourish the brain.
The picture shows the membranes of the brain
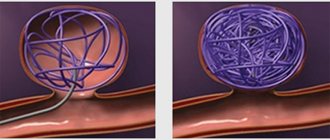
As a result of infection, an inflammatory process occurs, which leads to clouding of the membrane and the appearance of compactions in it. Thus, adhesions appear between the arachnoid membrane and the blood vessels, interfering with fluid circulation. Gradually, cysts appear here.
Inflammation of the arachnoid membrane leads to increased intracranial pressure due to:
- Disorders of fluid outflow.
- Impaired absorption of cerebrospinal fluid through the outer membrane of the brain.
With an autoimmune disease, it is possible to produce antibodies that have an inhibitory effect on the tissue of the arachnoid membrane. In this case, the inflammatory process can occur only in this one membrane. This condition is usually called true arachnoiditis.
Georgy Aleksandrovich Ermakov, an immunologist at the Moscow Doctor clinic, will tell you more about the pathology, its symptoms, risk groups and treatment methods:
If the disease occurs after an injury or infection, then this condition is called residual. Most patients are young people under 40 years of age. Children, people with weakened immune systems, metabolic disorders, and those suffering from alcohol or drug addiction are also at risk. Moreover, men are susceptible to the disease 2 times more often than women.
Symptoms
The first manifestations of symptoms may vary. The disease proceeds subacutely, becoming chronic, and has several types, the general symptoms of which are divided into the following:
- Severe headaches.
- Nausea and vomiting.
- Dizziness.
- Memory loss.
- Irritability.
- Disturbed sleep.
- Loss of performance.
- Decreased vision.
- Symptoms of nausea and vomiting occur with headaches, which most often begin in the morning.
The fact that the listed problems occur one or two weeks after the illness may also be one of the symptoms.
Depending on the area where the inflammatory process occurs, arachnoiditis can be divided into the following types, with their own symptoms:
Cerebral
It is an inflammation of the arachnoid membrane of the brain. Headaches with cerebral arachnoiditis are of a meningeal or hypertensive nature; they occur after physical and mental work, excessive cooling or overheating.
Optical-chiasmatic
Opticochiasmatic arachnoiditis affects the chiasmatic region of the brain after viral sinus infections or traumatic brain injury. Accompanied by pain in the back of the head with dizziness, nausea and vomiting, hearing loss, deterioration of the vestibular apparatus. Congestion is diagnosed in the fundus.
Adhesive
Adhesive arachnoiditis is an inflammation of the arachnoid membrane, which differs from cerebral arachnoiditis in the form of pus discharge. The resulting adhesions cause intense headaches.
Cystic
Cystic arachnoiditis involves the development of cysts due to inflammation of the arachnoid membrane and is also accompanied by headaches.
Cystic-adhesive
Cystic-adhesive inflammation in certain areas of the brain with adhesion. During mental and physical stress, symptoms appear in the form of seizures due to irritation of the cerebral cortex and subsequent fainting. In addition to the main symptoms, there are others: metabolic disorders, diabetes insipidus and obesity.
Treatment methods for inflammation of the lining of the brain
When the first signs of brain inflammation appear, you should immediately call an ambulance. In this condition, the person is sent to the intensive care unit of the hospital.
The following procedures will help confirm the diagnosis:
1. Blood and urine tests.
4. Examination of the brain fluid will make it possible to study the extent of the disease, identify its form and cause.
Treatment of such inflammation is always selected for each patient individually, depending on the type of pathology, its cause and form of progression.
Traditional therapy includes the following:
1. If the brain is damaged by bacteria, strong antibiotics are prescribed. They need to be injected within ten days. Types of antibiotics are selected depending on the causative agent of the disease.
2. In case of viral infection, treatment is carried out based on the symptoms (headaches, diarrhea and other symptoms are eliminated).
3. Diuretic medications are used to relieve brain swelling.
4. Albumin or isotonic solution can be used to reduce intoxication.
5. Glucocorticosteroids are used to prevent progression of edema.
6. If the disease is caused by fungi, then antibiotics will be ineffective. In this condition, the patient needs to be prescribed antimycotic drugs.
7. Antiviral medications are prescribed for rapid viral infections. Typically, the drug Cytosine arabinosis is used for this purpose.
8. Gammaglobulin is a central and essential drug for brain inflammation. It has a pronounced therapeutic effect and must be administered intravenously for three days.
9. If seizures or epileptic seizures are observed, anticonvulsant drugs are used.
10. In case of high temperature and fever, antipyretic drugs are prescribed.
It is important to know that meningitis and encephalitis are categories of diseases that require careful monitoring during treatment and reasonable selection of drugs. For this reason, self-medication when diagnosing such pathologies is strictly contraindicated.
Diagnostics
When diagnosing, the first step is to exclude brain tumors, since their symptoms are similar, but the treatment method is different. Due to the identified symptoms, the patient is prescribed magnetic resonance imaging (MRI). This diagnosis makes it possible to identify atrophic changes, the presence of cysts and other consequences of arachnoiditis, and to exclude hematoma, tumor and abscess.
MRI diagnostics is not the only one, since it does not allow identifying the disease in the initial stage. An integrated approach is used with analysis of disease history, symptoms and other diagnostic methods:
- Electroencephalography (EEG) – to detect epileptic activity.
- Examination of the fundus allows you to see congestion.
- Threshold audiometry is aimed at identifying the degree of hearing loss.
- Electrocochleography – to determine hearing damage.
- Lumbar puncture – may be needed to determine accurate intracranial pressure.
- The study of cerebrospinal fluid provides general indications that allow it to be separated from other cerebral diseases.
In addition to MRI, computed tomography may be prescribed. Diagnosis may take time. It is very important to identify the cause of the disease, since all subsequent treatment depends on it.
Diagnosis and treatment of inflammation of the meninges
Inflammation of the meninges and brain is diagnosed only when a sample of the cerebrospinal fluid - that is, an increased protein content and the number of white blood cells are detected.
Causal treatment is used, which consists in eradicating the pathogen that caused the disease. Therefore, antimicrobial drugs (antibiotics, for example penicillin, aminoglycosides, third generation cephalosporins), antituberculosis and antifungal drugs are used. In the case of a viral infection, it is impossible to eliminate the cause, so symptomatic treatment is prescribed, and in extremely severe cases, antiviral drugs and interferon.
Treatment
After confirming the diagnosis, the patient is admitted to the hospital. The treatment method depends on the degree of the disease and its characteristics. First of all, they start with eliminating the cause of arachnoiditis, treating otitis media, meningitis or other previous diseases. If treatment is started on time, the consequences can be easily avoided, otherwise the prognosis may be disastrous. The disease becomes chronic and causes death.
An integrated approach to treatment may include:
- Anti-inflammatory drugs - to eliminate the inflammatory process.
- Glucocorticosteroid therapy - can stimulate the immune system, improve the anti-inflammatory process and reduce allergic reactions.
- Absorbable agents – help improve blood circulation.
- Antiepileptic drugs - used for convulsive conditions.
- Dehydration drugs - to reduce intracranial pressure.
- Neuroprotectors and metabolites - help normalize brain metabolism.
- Antihistamines - to suppress allergic reactions to medications.
- Psychotropics are necessary to normalize the mental state.
The list of possible drugs is not limited to this, since it depends on the individual characteristics of the disease.
Surgery is usually aimed at separating adhesions or removing cysts that have a compressive effect on the areas of the brain where they are located. Indications for surgical intervention may include:
- Severe optico-chaosmal arachnoiditis.
- Arachnoiditis of the posterior cranial fossa with a sharp decrease in vision.
- Other cases are in advanced condition.
After treatment, the patient must adhere to a number of precautions: Avoid infectious diseases by strengthening the immune system. Refuse to work in noisy rooms and in conditions that differ significantly from the usual atmospheric pressure. Neglecting these rules can lead to recurrence of the disease.
Features of the treatment of inflammation of the lining of the brain
In addition to traditional drug therapy, the following procedures may be prescribed to a patient with brain inflammation:
1. Peloid therapy or mud treatment. This procedure is aimed at stimulating the nervous system, producing hormones, enhancing carbohydrate metabolism and restoring lipid metabolism.
The duration of the procedure should be twenty minutes. The course of treatment includes twelve sessions.
2. Thalassotherapy or taking baths with the addition of beneficial chemicals (iodine, calcium, potassium, etc.). These microelements will penetrate the skin through the sweat glands and enter the blood. Thanks to this procedure, it is possible to improve microcirculation in tissues, restore brain dynamics and relieve inflammation.
Consequences of the disease and further prognosis
Treatment can be difficult and take a long time. Diagnosing arachnoiditis is quite a difficult task, despite modern technology. Since the prognosis depends on the stage at which the disease is detected, it is very important to seek the help of specialists immediately when the first symptoms appear. When diagnosed at the initial stage, at the first symptoms, in childhood, recovery can be complete.
An injured person may be recognized as disabled:
- The third group is assigned when there is a decrease in working capacity.
- The second group is with significant vision loss and the presence of epileptic seizures.
- The first group includes people with vision loss, the cause of which is opticochiasmatic arachnoiditis.
The prognosis for life with proper treatment is also favorable. Exceptions may be arachnoiditis of the posterior cranial fossa with occlusive hydrocephalus.
Causes of inflammation of the meninges and brain
Inflammation of the brain and meninges can be caused by many bacteria, viruses or fungi. The viruses that most commonly cause meningitis include enteroviruses, arthroponosis viruses, ECHO viruses, HSV-2, Coxsackie virus, polio virus, influenza A and B virus, or measles virus.
Among bacteria, the most cases of brain inflammation were recorded as a result of infection with Neisseria meningitidis (diplococcus), Streptococcus pneumoniae (pneumococcus), Haemophilus influenzae type B, among fungi - Cryptococcus neoformans, Coccidioides immitis.
The main cause of etiological encephalitis are neurotropic viruses. The most common, vesicular inflammation of the brain, is caused by the herpes virus. Inflammation of the brain can also be caused by certain protozoa.
Non-infectious causes of inflammation of the meninges and brain include tumors (leukemia, lymphatic cancer, brain tumors, brain metastases), sarcoidosis, lead poisoning, and the use of certain medications, such as methotrexate.
Complications
In the absence of the necessary treatment for inflammatory processes in the brain, the following pathologies may develop:
- Paralysis.
- Visual impairment.
- The appearance of epileptic seizures.
- Kidney and liver failure develops.
- Dysfunction of the musculoskeletal system.
- Strabismus.
- Memory and hearing impairment.
- Cardio muscle function deteriorates.
The main complication of brain inflammation is the death of the patient. It occurs if the patient is not treated within five to eight days after the disease begins.
Course of therapy
Elimination of inflammation of the arachnoid membrane occurs step by step:
- First stage. Initially, the underlying disease is treated. For this purpose, drugs are used to eliminate the cause of the disease. Usually the doctor prescribes antibiotics and antiallergic medications (Diphenhydramine, Diazolin);
- Second phase. After eliminating the cause of the pathology, the doctor will adjust the treatment to reduce the pressure inside the skull and normalize the circulation of blood and cerebrospinal fluid. Typically, stimulants and iodine medications (Potassium Iodide, Lidaza) are used for this purpose.
During the main course of therapy, the attending physician will prescribe diuretics and anti-ophthalmic medications (Frusemide, Glycerin) to reduce the amount of accumulated fluid in the brain. If the patient experiences seizures, then antiepileptic medications are added to the treatment regimen.
For spinal arachnoiditis, surgery is sometimes used to remove adhesions and cysts. This radical method of therapy is required mainly for cystic and cystic-adhesive types of the disease.
Inflammation of the membranes of the brain is a severe pathological process, which is characterized by various symptoms.
The severity of the disease directly depends on its form and the location of the source of inflammation. However, it is treatable, especially in the early stages, so it is advisable not to delay a visit to the doctor in order to undergo a course of therapy in a timely manner. -
inflammation of the meninges. The disease is caused by various bacteria, viruses, rickettsia, and fungi. The soft and arachnoid membranes and the closely associated choroid plexuses of the ventricles become inflamed.
With meningitis, the absorption and circulation of cerebrospinal fluid is impaired, which leads to the development of intracranial hypertension. The process may involve the substance of the brain and spinal cord, roots, cranial nerves, and cerebral vessels. Primary meningitis occurs as an independent disease, while secondary meningitis is a complication of somatic diseases.
Symptoms of meningitis
Meningitis is characterized by meningeal syndrome: vomiting, stiffness of the neck muscles, Kernig and Brudzinski symptoms, general hyperesthesia, high temperature, inflammatory changes in the cerebrospinal fluid.
Depending on the nature of the disease and its stage, the severity of individual symptoms varies widely. The diagnosis of meningitis is based on the characteristics of the clinical picture and the composition of the cerebrospinal fluid, as well as on data from its bacteriological and virological examination.
Meningism is an irritation of the meninges without penetration of infection into the subarachnoid space (the composition of the cerebrospinal fluid is normal), often observed at the height of general diseases accompanied by intoxication and high fever. Depending on the composition of the cerebrospinal fluid, meningitis is divided into purulent and serous.
- Purulent meningitis is characterized by the presence of neutrophilic pleocytosis in the cerebrospinal fluid, exceeding 500 cells per cubic meter. ml. Purulent meningitis can be caused by various pathogens: meningococci, pneumococci, Haemophilus influenzae, streptococci, Escherichia coli, etc.
Meningococcal meningitis - see Meningococcal infection.
Pneumococcal meningitis mainly affects young children and people over 40 years of age (in the latter it is the most common form of purulent meningitis). Sources of infection and factors contributing to the transition of lesions to the membranes of the brain are chronic otitis and sinusitis, mastoiditis, skull injuries, alcoholism, and immune disorders. As with meningococcal meningitis, there may be prodromal symptoms in the form of general malaise and low-grade fever. Skin rashes are uncommon, with the exception of herpes labialis. The clinical picture is typical of severe bacterial meningoencephalitis. Characterized by short-term loss of consciousness, convulsions and paralysis of the cranial nerves. The greenish color of turbid cerebrospinal fluid is very typical. Without treatment, the disease leads to death after 5-6 days, however, even with adequate treatment, the mortality rate is high (up to 50%).
Treatment of meningitis
Identification of the pathogen by bacteriological examination, which sometimes requires a long time, is possible only in 70-80% of cases. In the most acute stage, many sporadic cases of purulent meningitis do not have sufficiently convincing etiological signs, therefore, first of all, penicillin is prescribed at the rate of 200,000-300,000 units/kg, and for infants 300,000-400,000 units/kg per day, which is on average for adult patients 24,000,000 units/day.
- Penicillin is administered at 4-hour intervals (6 times a day) in adults and at 2-hour intervals in infants. Higher doses of penicillin are only necessary if treatment is started late or if symptoms of meningoencephalitis are obvious. In such cases, along with intramuscular administration, intravenous administration of benzylpenicillin sodium salt is also indicated - from 4,000,000 to 12,000,000 units/day.
Instead of benzylpenicillin, semi-synthetic penicillins - ampicillin sodium salt, oxacillin, methicillin - can be used for purulent meningitis. Ampicillin is administered 2 g every 4 hours IM or IV (up to 12 g/day), for children - 200-400 mg/kg IV every 6 hours.
Sometimes iv administration of sulfamone methotoxin is added to penicillin on the 1st day, 2 g 2 times, and on subsequent days, 2 g 1 time per day.
If you are intolerant to penicillin, use gentamicin (up to 5 mg/kg per day), chloramphenicol (up to 4 g/day), vancomycin (up to 2 g/day). Cephaloridine (ceporin) has a wide spectrum of action.
The optimal range of antibiotics is as follows: meningococcus, pneumococcus - benzylpenicillin, or amoxicillin, or chloramphenicol, or cephaloridine (6 g/day); Afanasyev-Pfeiffer stick - ampicillin and chloramphenicol.
Combined treatment of meningococcal meningitis with several antibiotics has no advantage over massive doses of penicillin or ampicillin. However, for meningitis caused by Haemophilus influenzae, it is necessary to combine ampicillin and chloramphenicol, if E. coli is detected in the cerebrospinal fluid - ampicillin and gentamicin, if streptococcus is detected - penicillin and gentamicin. In severe cases, penicillin, gentamicin or streptomycin are added intralumbarally. In severe cases, immediate plasmapheresis is required, followed by the administration of fresh frozen plasma up to 1-2 liters (dose for adults).
Serous meningitis is characterized by lymphocytic pleocytosis within several hundred cells in 1 μl
Tuberculous meningitis
Tuberculous meningitis in most cases develops gradually, manifested by an increasing headache against a background of low fever, which is only followed by vomiting, adynamia, and stupor after a few days. At the beginning of the 2nd week of the disease, damage to the cranial nerves, usually the oculomotor and (or) abducens, is detected; at the end of the 2nd week, pelvic organ dysfunction and confusion occur. In half of the cases, tuberculous meningitis occurs against the background of an active tuberculosis process, most often in patients with hematogenously disseminated pulmonary tuberculosis. Currently, the disease is equally common in both children and adults. In the early stages of the disease, differentiating tuberculous meningitis from viral meningitis presents significant difficulties. Even minor signs of impaired oculomotor innervation and a decrease in glucose content in the cerebrospinal fluid are the most important arguments in favor of tuberculous lesions of the membranes.
Treatment of tuberculous meningitis
Isoniazid (tubazid) 0.3 g 3 times a day (adults), streptomycin intramuscularly once a day at a dose of 1,000,000 units, rifampicin. Atambutol is often additionally prescribed. Chemotherapy drugs are combined with glucocorticoid hormones - 15-30 mg/day of prednisolone orally. In cases of meningoencephalitis, intensive therapy for cerebral edema is necessary. To prevent polyneuropathy and seizures sometimes caused by tubazide and its analogues, vitamin B6 and phenobarbital are prescribed.
Forecast. With timely initiation of treatment, which lasts many months, as a rule, complete recovery occurs. In case of delayed diagnosis, especially if blackouts, focal brain lesions and hydrocephalus are observed, the outcome is unfavorable, and among those who survive, the majority have residual symptoms.
Viral meningitis
Causative agents of viral meningitis: Coxsackie viruses, ECHO, benign lymphocytic choriomeningitis and mumps; serous meningitis can be caused by any other neurotropic virus, when at the height of viremia the membranes of the brain are involved in the process. Outside of an epidemic outbreak, the clinical picture of aseptic meningitis, as a rule, is not specific.
The disease begins acutely or subacutely: with a moderate increase in temperature, headache, vomiting, general malaise, tension in the neck muscles and Kernig's sign appear. Significant signs of general intoxication are usually not observed. Pharyngitis is not uncommon. There are no blood changes. In the cerebrospinal fluid, lymphocytic pleocytosis is noted with a slight increase in protein with normal glucose levels. Among viral meningitis, the most important is meningitis (or meningoencephalitis), which occurs in 0.1% of cases of mumps. Neurological syndrome develops 3-6 days after the onset of the disease. Occasionally, mumps meningitis takes a severe course, accompanied by brain damage. When treating patients with mumps meningitis, one should remember the possibility of developing polyneuropathies, isolated damage to the auditory nerve, as well as concomitant damage to the pancreas (abdominal pain) and gonads (orchitis).
Treatment of viral meningitis
Treatment is symptomatic: analgesics, diuretics, tranquilizers, antihistamines, bed rest. The vast majority of patients with aseptic meningitis are subject to hospitalization in infectious diseases departments due to the high contagiousness of enteroviral infections. Forecast. In most cases, recovery occurs within a few days or weeks.
Meningitis is an inflammation of the meninges. The cause of conquest can be bacteria, fungi, protozoa, or viruses. There are primary and secondary meningitis. In primary meningitis, inflammation of the meninges is not preceded by diseases of any other organs. Secondary meningitis occurs as a complication of other diseases (inflammation of the middle ear cavity, purulent processes in the face and head, traumatic brain injury, tuberculosis, mumps, etc.). According to the clinical course, meningitis is divided into fulminant, acute, subacute and chronic. The course of meningitis depends on the nature of the pathogen, the reactivity of the body, and the age of the patient.
The main clinical manifestation of meningitis is meningeal (meningeal) syndrome, which includes headache, vomiting, general hyperesthesia, specific posture of the patient and a number of other symptoms.
The headache is usually diffuse and occurs at any time of the day. It is caused by toxic and mechanical (due to increased intracranial pressure) irritation of the receptors of the meninges. The headache is accompanied by vomiting, which occurs suddenly or against the background of previous nausea. Vomiting is not associated with food intake and brings some relief.
General hyperesthesia is observed. The patient is extremely uncomfortable with touching the skin, visual and auditory influences. The basis of general hyperesthesia is mechanical irritation of the sensory roots of the spinal and cranial nerves by the cerebrospinal fluid overflowing the subarachnoid space.
The posture of patients with meningitis is characteristic: the head is thrown back, the torso is arched, the stomach is retracted, the arms are bent, pressed to the chest, the legs are pulled up to the stomach (Fig. 87, a). This position of the patient is a consequence of reflex tonic muscle tension. This mechanism underlies other meningeal symptoms. Rigidity of the neck muscles is detected when trying to bend the patient's head to the chest (Fig. 87, b).
Let's name the symptoms observed with meningitis. Kernig's symptom is the inability to straighten a leg at the knee joint that is previously bent at the hip and knee joints (Fig. 87, c).
A - posture of a patient with meningitis; b — muscle tension in the back of the head and the upper Brudzinski’s sign; c — Kernig’s sign and lower Brudzinski’s sign
The upper Brudzinsky symptom is involuntary flexion of the legs at the knee and hip joints when bringing the patient's head to the chest (Fig. 87, b).
The lower Brudzinski symptom is involuntary flexion of one leg at the knee and hip joints while extending the other (Fig. 87, c).
The symptom of Lesage hanging is determined in young children: the child, raised under the armpits, pulls his legs towards his stomach and holds them in this position for some time (Fig. 88).
Bekhterev's symptom is a grimace of pain on the corresponding half of the face, which occurs when tapping on the zygomatic arch. A symptom of sitting up is the inability to sit in bed with straight legs.
The most constant and obligatory sign of meningitis is inflammatory changes in the cerebrospinal fluid, characterized by an increase in the number of cells and a moderate increase in protein content (protein-cell dissociation). Changes in the cerebrospinal fluid make it possible to diagnose meningitis even in the absence of pronounced meningeal symptoms, as is often the case in young children (clinically asymptomatic, liquor-positive meningitis).
Depending on the nature of the inflammatory process and changes in the cerebrospinal fluid, meningitis is divided into purulent and serous.
Purulent meningitis is caused mainly by bacteria - meningococcus, pneumococcus, staphylococcus, streptococcus, Escherichia coli, Proteus, Pseudomonas aeruginosa, etc. In purulent meningitis, the meninges are saturated with serous-purulent effusion, located on the convex surface of the brain and its base. If no treatment is carried out, then by the 4th -8th day the purulent effusion thickens, settles on the meninges and changes their structure. Inflammation can spread to the membranes of the spinal and cranial nerves, the inner lining of the ventricles, the substance and vessels of the brain. Pathological changes in the meninges, if untimely and incorrectly treated, can lead to blockage of the cerebrospinal fluid spaces, disruption of the production of reabsorption of cerebrospinal fluid, and the development of hydrocephalus. Meningeal syndrome with purulent meningitis usually develops against the background of pronounced signs of intoxication, i.e. poisoning with poisons and other waste products of bacteria. Such signs include increased breathing and heart rate, lack of appetite, pallor or grayish tint of the skin, cyanosis of the nasolabial triangle, anxiety or lethargy, and indifference of patients. With erased, abortive forms of purulent meningitis, symptoms of general intoxication may come to the fore. In an acute and fulminant course, due to the development of cerebral edema, sometimes in the first hours of the disease disturbances of consciousness and convulsive attacks may be observed. Such seizures sometimes develop into status epilepticus, a condition in which seizures follow one another.
Secondary forms of purulent meningitis are accompanied by clinical symptoms due to a specific localization of the primary infectious focus. Symptoms such as severe respiratory failure due to pneumococcal disease, severe diarrhea (diarrhea) and exicosis (dehydration) due to E. coli infection can be mentioned. Extrathecal symptoms also include various kinds of skin rashes, which may be the result of toxic paresis of small vessels of the skin or their bacterial embolism (Fig. 89).
In the blood with purulent meningitis, significant leukocytosis (3.0-109/l or more) and an increase in erythrocyte sedimentation rate (ESR) are observed. The cerebrospinal fluid is turbid, purulent, and milky white. The number of cells reaches several thousand in 1 mm3, of which 70-100% are neutrophils. The protein content is slightly increased. The amount of sugar is normal or reduced. The form of purulent meningitis is determined by bacteriological examination of cerebrospinal fluid.
The course of purulent meningitis and the nature of the consequences largely depend on the timeliness and nature of the treatment. With early and rational therapy, the condition of patients improves significantly on the 3rd - 4th day of illness; complete normalization occurs by 8–15 days. In these cases, after purulent meningitis, children may experience mildly expressed residual effects in the form of increased excitability and exhaustion of the nervous system, emotional instability, impaired concentration, and hydrocephalic syndrome. With a late diagnosis and improper therapy, a protracted course of purulent meningitis is possible, leading to gross disturbances in the structure of the meninges, discirculation of cerebrospinal fluid and other complications. An increase in the secretion of cerebrospinal fluid, a violation of its reabsorption, as well as disorders that prevent its normal movement in the ventricular system and sub-arachnoid space are the causes of the development of hydrocephalus. Hydrocephalus is most often observed with meningitis in young children. Approximately 20% of children who have suffered purulent meningitis show signs of focal damage to the nervous system: epileptiform convulsions, convergent and divergent strabismus, paresis of the facial nerve, deafness, autonomic-metabolic disorders, motor disorders, mental retardation.
Serous meningitis is caused mainly by viruses. Pathomorphological changes in them are less severe than in purulent meningitis. A serous inflammatory process is observed in the meninges, the main characteristics of which are swelling and congestion of the blood vessels. In the clinical picture of serous meningitis, in contrast to purulent meningitis, signs of intoxication are less pronounced. The leading symptoms are increased intracranial pressure: frequent vomiting, headache, agitation, anxiety. Lethargy, adynamia, and lethargy are less common.
The pressure in the cerebrospinal fluid is increased. It flows out in frequent drops or streams. The liquid is colorless, transparent. Its cellular composition is represented mainly by lymphocytes, the number of which ranges from several tens to several hundred per 1 mm3. Lumbar puncture for serous meningitis usually brings relief to patients. Serous meningitis, as a rule, does not leave significant consequences. For some time, headaches, increased fatigue, emotional lability, and rapid exhaustion of the nervous system may be observed. Treatment of meningitis in the acute period should begin as early as possible and be carried out in a hospital under the supervision of medical personnel. For all forms of purulent meningitis, antibacterial therapy is prescribed. The use of a particular tibiotic depends on the type of pathogen. Before determining the nature of the pathogen, so-called urgent (urgent) antibacterial therapy is carried out. For meningococcal meningitis, they begin with the prescription of penicillin, which in 90% of cases is an effective treatment. Penicillin is used in large doses, depending on the age and body weight of the child. Penicillin is administered at short intervals (2-3) in order to maintain its therapeutic concentration in the blood. If the type of pathogen is established, then you need to use those antibiotics to which the bacteria are more sensitive. Along with antibacterial agents, agents are used that reduce cerebral edema and intracranial pressure, relieve nonspecific allergic reactions, normalize blood circulation, acid-base status and mineral metabolism, antipyretics, etc. The outcome of the disease and the nature of the residual effects depend on how early the treatment is started and how rationally the treatment is carried out. A child who has had meningitis needs a gentle health regime, healthy sleep, time in the fresh air, and good nutrition. A child’s activities should not be monotonous for a long time. It is necessary to alternate mental and physical activities. The child should be given vitamins, as well as drugs that improve metabolism in the brain tissue and increase the supply of oxygen to the brain.
Among viruses, these are most often the causative agents of mumps, measles and rubella, spring summer encephalitis, HIV and herpes simplex virus.
Pathogens usually enter the brain through the bloodstream. However, infection can also penetrate from neighboring areas (for example, with inflammation of the middle ear and paranasal sinuses). Severe head injuries can also contribute to the development of meningitis.
Symptoms (complaints)
Important: If you experience severe headaches, high fever, stiff neck and a sharp deterioration in your overall health, you must urgently call a doctor or emergency service (phone number 144).
- Rigidity of the neck (doctors in this case talk about meningism)
- Headache
- High body temperature (39-40 ° C)
- Poor health in general
- Vomiting, diarrhea (often with viral nature of meningitis)
- Photophobia
- When the disease is severe: loss of consciousness, confusion, seizures, coma.
- Warning signs: the appearance of multiple bluish spots, dark spots or large patchy areas on the skin (minor bruising)
- In infants and small children, complaints are often less pronounced:
they become sleepy, behave sluggishly when feeding, seem to be “cranky,” have a bad mood, and in some cases even have convulsions.
Diagnostics (research)
- During the examination, the doctor determines whether there are manifestations of meningism
- Examination of cerebrospinal fluid (lumbar puncture): to diagnose infection and determine the presence of a pathogen in the brain fluid
- Blood test: to confirm inflammation and the presence of a pathogen
Therapy (treatment)
Inflammation of the meninges is a very dangerous disease that, if left untreated, leads to death. Therefore, prompt hospitalization and immediate treatment are vital factors.
For meningitis caused by a bacterial infection, antibiotic therapy is given. If there is even the slightest suspicion of inflammation of the meninges, the family doctor will immediately prescribe therapy. The earlier the better!
If the disease is caused by viruses, then symptomatic therapy is carried out (to eliminate the main symptoms - headache, fever, diarrhea, etc.). In doubtful cases, it is important to remember: treatment must begin before the final diagnosis is made!
Possible complications
Without treatment, meningitis is fatal. Early diagnosis and immediate initiation of therapy are vital. As a rule, treatment is started by a family doctor; if this is not possible, then the latest date for therapy is the moment of admission to the clinic. Further complications include inflammation of the medulla and brain abscess. When treating an abscess, surgical intervention is necessary, in which the inflammatory focus is removed along with the capsule, then antibiotics are prescribed. And yet, despite the therapy, 20% of patients die.
Inflammation of the meninges and brain can be formed under the influence of factors such as bacteria (meningococci, pneumococci), viruses and protozoa. Depending on the factor causing the development of the disease, it can be unexpected and very violent (meningococci) or slowly progressive and hidden (tuberculosis).
Brain inflammation can also be caused by non-infectious factors, which include brain tumors, leukemia, lead poisoning, or a drug such as methotrexate.